For a health system, the practical question behind AI-assisted wildfire preparedness for health is not whether an algorithm can draw a prettier smoke plume. It is which patients should be contacted first before smoke arrives, and what makes that prioritization defensible. A ranked list that names only “high-risk patients” is not enough. The list has to say whether risk comes from severe asthma, pregnancy, age, likely indoor exposure, delayed evacuation, lack of filtered air, or a neighborhood already carrying other pollution burdens.
That distinction matters because wildfire preparedness is becoming a health system performance problem, not only an emergency management problem. A 2024 Lancet Planetary Health article framed wildfire readiness as work that must happen before, during, and after fires, including planning for continuity of care, patient protection, facility operations, and recovery rather than treating smoke as a short-lived environmental inconvenience.[1]
The Useful Output Is Not a Forecast. It Is an Outreach Queue.
Smoke forecasting still matters. Clinics cannot prepare staffing, call scripts, medication refills, indoor air guidance, or shelter coordination without some expectation of timing and location. But for population health teams, the operational product is more specific: a stratified queue of people who may need outreach before the air quality index turns dangerous.
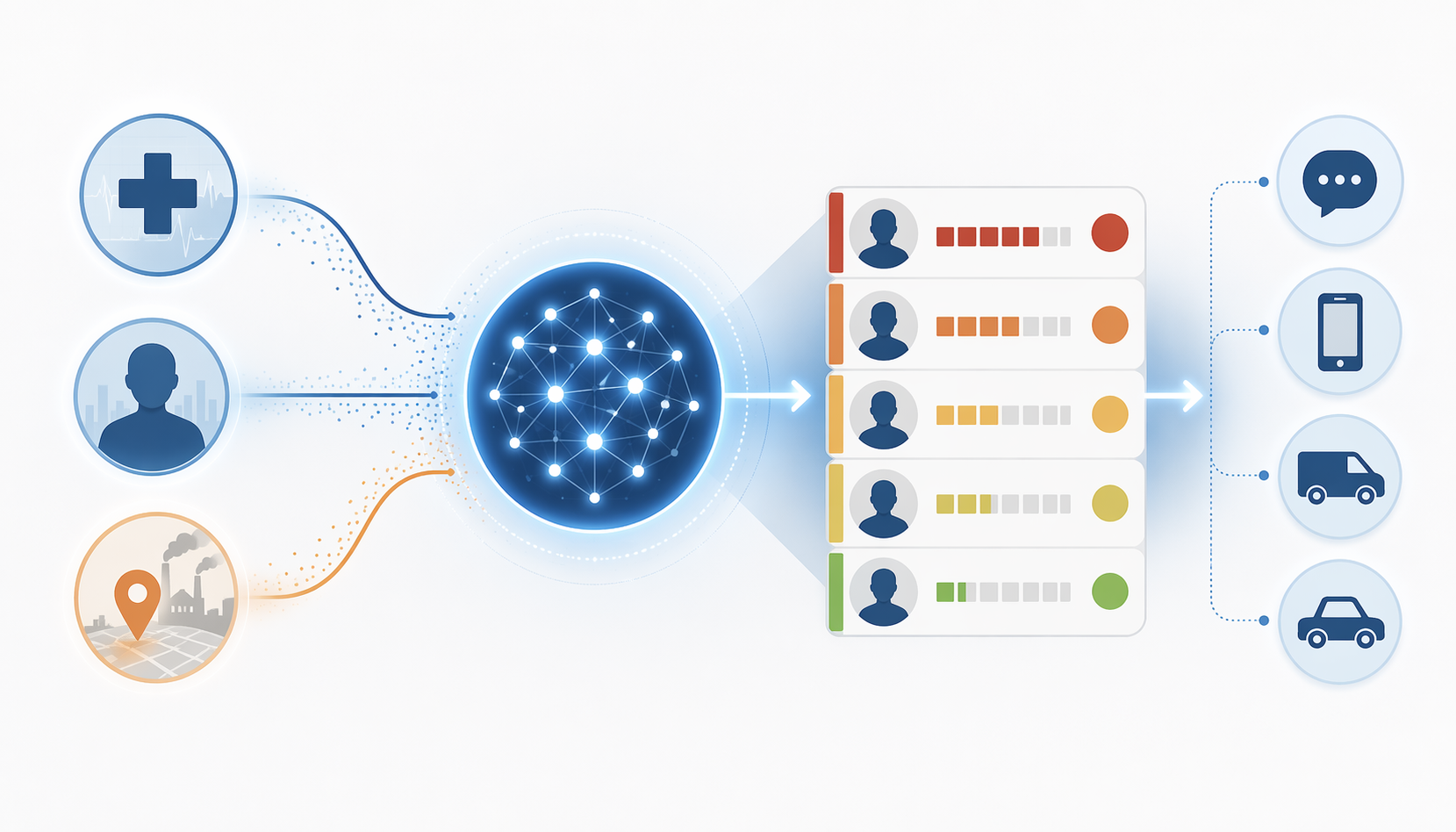
An AI-assisted workflow for wildfire smoke vulnerability would usually combine three kinds of signals. Clinical data identify people more likely to be harmed by smoke exposure. Environmental data identify where exposure may be more intense or compounded by other hazards. Behavioral or social data estimate whether warnings are likely to turn into protective action. The model’s job is to help decide where limited staff time goes first.
| Layer | What It Can Add | What It Cannot Prove |
|---|---|---|
| Clinical risk | Identifies patients whose age, diagnosis, pregnancy status, medications, or prior utilization suggest higher vulnerability to smoke exposure. | That AI-targeted outreach will prevent emergency visits, preterm birth, cognitive decline, or death. |
| Environmental exposure | Highlights communities where smoke may combine with traffic, industrial, mining, or hazardous waste burdens. | That every patient in a high-burden geography has the same individual risk or the same ability to act. |
| Behavioral risk | Estimates who may delay evacuation, miss warnings, or be unable to reach safer indoor air. | That predicted behavior will match real behavior during a specific fire. |
| Outreach operations | Turns stratification into texts, calls, transportation support, medication checks, or facility air-quality planning. | That the intervention works unless outcomes are prospectively evaluated. |
That last column is the evidence boundary. Current evidence supports using AI and adjacent analytic methods to find risk more precisely. It does not yet show that AI-guided wildfire outreach improves clinical outcomes during real smoke events.
Clinical Risk Has to Be Broader Than the Usual Smoke Alert List
The first version of a wildfire smoke list is predictable: older adults, people with asthma or chronic obstructive pulmonary disease, people with cardiovascular disease, and patients dependent on oxygen or frequent respiratory medications. That is a reasonable starting point. It is also too narrow if the goal is to identify patients whose risk may be missed until the call center is already saturated.
Smoke exposure has been associated with cardiopulmonary harm, but the risk picture now reaches into pregnancy, childhood development, and cognition. Stanford’s summary of wildfire health evidence notes that children can show reduced lung function 2 to 4 years after wildfire exposure, and that pregnant women face elevated risk of preterm birth.[2] The Harvard Salata Institute similarly describes health effects occurring now, soon, and later rather than only during the visible smoke episode.[3]
The older-adult dementia signal deserves attention, but also restraint. A study of 1.2 million older adults, presented at the Alzheimer’s Association International Conference in 2024 and reported by Stanford and Harvard, found a 21% increase in dementia risk per 1 µg/m³ rise in wildfire-related PM2.5, compared with a 3% increase per 3 µg/m³ rise in PM2.5 from other sources.[2][3] Because that figure is being used here through institutional reporting of a conference presentation, not a fully appraised primary paper in the materials available for this article, it should be treated as an important signal to verify rather than as settled clinical guidance.
Even with that caveat, the signal changes how a preparedness list should be built. A patient with dementia risk factors, frailty, limited mobility, or caregiver dependence may not fit the classic “respiratory patient” filter. A pregnant patient living near a high-pollution corridor may need earlier outreach than a healthier patient in the same smoke plume. A child with prior wildfire exposure may not be visible in adult-centered utilization data. AI can help assemble these overlapping signals, but only if the health system chooses to feed the model more than diagnosis codes for asthma and COPD.
What a Clinically Useful Stratification Model Would Need
- Age and frailty markers, including older adults who may have cognitive impairment, mobility limits, or caregiver dependence.
- Respiratory and cardiovascular diagnoses, prior exacerbations, oxygen dependence, and medication refill gaps.
- Pregnancy status and pediatric risk, especially when exposure may overlap with poor housing or high-pollution geography.
- Communication reliability, such as whether the patient responds to portal messages, texts, or phone calls.
- Likely access to protective conditions, including filtered indoor air, transportation, and a caregiver who can act on instructions.
The communication fields are not administrative trivia. A patient who opens every portal message and has a working air purifier is operationally different from a patient at the same clinical risk level who does not answer texts and lives alone. The model can rank both as vulnerable; the outreach plan should not treat them the same.

Environmental Justice Data Change Who Moves Up the List
A smoke map can make exposure look evenly distributed across a county. Patient experience rarely works that way. Indoor air quality, housing conditions, traffic corridors, industrial sites, work requirements, language access, and transportation all shape whether a smoke warning becomes actual protection.
Penn State researchers studying the 2023 Canadian smoke events found that communities already burdened by mines, heavy traffic, and hazardous waste sites experienced disproportionately amplified PM2.5 levels. Their improved smoke model was presented as a way to identify areas for public health intervention at the county level.[4]
For a health system, that finding has a direct consequence. A patient panel should not be sorted only by diagnosis severity. Geography can move people upward when smoke intersects with existing environmental burden. The patient with moderate asthma in a compounded-exposure area may warrant earlier contact than a patient with similar clinical history in a less burdened setting.
This is also where AI can be useful without being magical. Models can merge EHR-derived vulnerability with parcel, census, air quality, traffic, industrial, and emergency planning data. They can flag neighborhoods where clinics should prepare phone outreach, community health worker visits, medication refill campaigns, or coordination with local cooling and clean-air spaces. They cannot create those spaces, guarantee transportation, or make an under-resourced household able to shelter in filtered air.
Behavioral Models Address the People Who Do Not Follow the Clean Pathway
Preparedness plans often assume a simple chain: warning sent, patient understands, patient acts. Smoke seasons expose the weak points in that chain. Some people do not receive the alert. Some receive it but cannot leave work. Some distrust the instruction. Some wait because evacuation has costs they cannot absorb. Some have pets, medical equipment, mobility limits, or family obligations that make the recommended action unrealistic.
The FLARE project, led by Johns Hopkins and the University of Florida with a $1.2 million National Science Foundation grant, is using AI guided by behavioral and psychological theory to predict which populations are likely to wait, evacuate late, or not evacuate at all during wildfires.[5] The project is research-stage; the available material does not show deployment in an active wildfire evacuation or prospective proof that it improves outcomes.
Still, the planning value is concrete. If a model can identify groups likely to delay evacuation or miss protective actions, a health system can shift from generic mass messaging to differentiated outreach. One group may need early phone calls in a preferred language. Another may need transportation coordination. A long-term oxygen patient may need durable medical equipment planning. A family with a medically fragile child may need instructions that account for school closures and indoor air filtration rather than a one-line warning to “stay inside.”
This is where the handoff from AI to people begins. The model can produce a prioritized worklist. Nurses, care managers, community health workers, and clinic operations teams decide what happens next: who receives a text, who gets a phone call, who needs a home health check, who needs medication refills before roads close, and who should be connected to transportation or cleaner indoor space.
Forecast Accuracy Is Necessary, but It Is Not the Whole Preparedness Problem
AI smoke forecasting and exposure models can help health systems anticipate where smoke may go. The hard limitation is that model performance can diminish during extreme wildfire events, which are exactly the conditions when operational decisions become urgent. Penn State’s work on improved smoke modeling is valuable because it connects smoke prediction to public health intervention zones, but it should not be read as proof that forecasts will be precise enough for every clinical action in every severe event.[4]
A practical system therefore should not wait for perfect plume prediction. It should use forecast confidence as one input among others. When the risk list is already known—older adults with respiratory disease, pregnant patients in high-burden corridors, children with prior exposure, oxygen-dependent patients, people unlikely to respond to digital alerts—some preparedness actions can begin before the exact smoke path is certain.
The Intervention Layer Is Where Evidence Thins Out
Health systems already have pieces of the intervention layer. The Lancet Planetary Health preparedness framework describes operational planning across wildfire phases, and some health systems already use opt-in text alerts for vulnerable patients during extreme heat and poor air quality events.[1] NOAA has also described how health care facilities maintain indoor air quality through smoke and wildfires, including facility-level planning rather than patient-level AI targeting.[6]
Those precedents make AI-assisted wildfire outreach plausible. They do not make it proven. A health system could use AI to identify high-priority patients, send air quality guidance, arrange earlier medication refills, advise on portable air cleaners, coordinate transport, or prepare clinic staff for respiratory demand. But the available evidence does not include prospective controlled trials showing that AI-stratified outreach during wildfire events reduces emergency visits, hospitalizations, preterm births, cognitive decline, or mortality.
That absence should shape implementation. AI wildfire preparedness should be treated as a population health targeting layer that requires evaluation, not as a turnkey clinical intervention. At minimum, health systems testing it should track who was identified, who was reached, what action was taken, whether high-risk groups were missed, and whether outreach differed by language, rurality, housing status, disability, or digital access.
A Defensible Workflow Before Smoke Arrives
- Build the registry before the season: cardiopulmonary disease, older age, pregnancy, pediatric vulnerability, frailty, oxygen dependence, prior utilization, and medication access.
- Add place-based exposure: smoke-prone areas, high-traffic corridors, industrial or hazardous waste burden, rural isolation, and access to cleaner indoor spaces.
- Add reachability: preferred language, portal use, text response, phone reliability, caregiver availability, transportation barriers, and prior missed outreach.
- Stratify into action groups, not just risk scores: digital message, nurse call, community health worker follow-up, refill support, transportation coordination, or facility-based planning.
- Audit the gaps: patients without phones, households without filtered air, rural patients beyond service reach, and groups whose risk is high but whose contact rate is low.
- Evaluate outcomes separately from identification: reach rate, action completion, emergency use, respiratory exacerbations, obstetric outcomes, and equity of intervention delivery.
The fourth step is often where a model-centered plan fails. A percentile score does not call a patient, refill an inhaler, fix indoor air, or drive someone to a safer location. If the output is not tied to a staffed action, the system has only improved its ability to describe risk.
What Can Be Said in Q3 2026
AI can help health systems move from a vague category of “vulnerable patients” to a more usable map of clinical, environmental, and behavioral risk. The strongest case is not that AI can solve wildfire health risk. It is that AI can help population health teams find patients and communities that a standard smoke alert strategy is likely to miss.
The evidence is strongest for risk identification: older adults, children, pregnant patients, people with cardiopulmonary disease, patients in compounded pollution environments, and groups likely to delay or be unable to act on evacuation and smoke warnings. The evidence is weakest at the point that matters most to patients: whether AI-guided outreach changes health outcomes during actual wildfire smoke events.
So the responsible conclusion is limited but useful. AI-assisted wildfire preparedness is credible as a population health targeting layer and promising as a way to organize proactive outreach. In Q3 2026, it remains unproven as an outcomes-improving clinical intervention during real wildfire events.
References
- Seasons of smoke and fire: preparing health systems for improved performance before, during, and after wildfires. The Lancet Planetary Health, 2024.
- What we know about the health effects of wildfire. Stanford Report.
- How exposure to wildfire smoke impacts human health now, soon, and later. Harvard Salata Institute.
- Improved wildfire smoke model identifies areas for public health intervention. Penn State / ScienceDaily, 2024.
- Researchers use AI tools to model, improve wildfire evacuation. Johns Hopkins Hub, 2026.
- Health care facilities maintain indoor air quality through smoke and wildfires. NOAA Climate.gov.
Comments
Join the discussion with an anonymous comment.