Hazardous air quality days in July 2026 have made air quality hazard levels and health risks feel less like an abstract environmental topic and more like a clinic question: when a patient sees the AQI turn orange, red, purple, or maroon, what should that patient actually do, and how much protection should a clinician imply that advice provides? Recent extreme AQI events have brought that question back into public view, especially for people with asthma, COPD, established cardiovascular disease, older age, pregnancy, outdoor work, or little control over indoor air quality.[1]
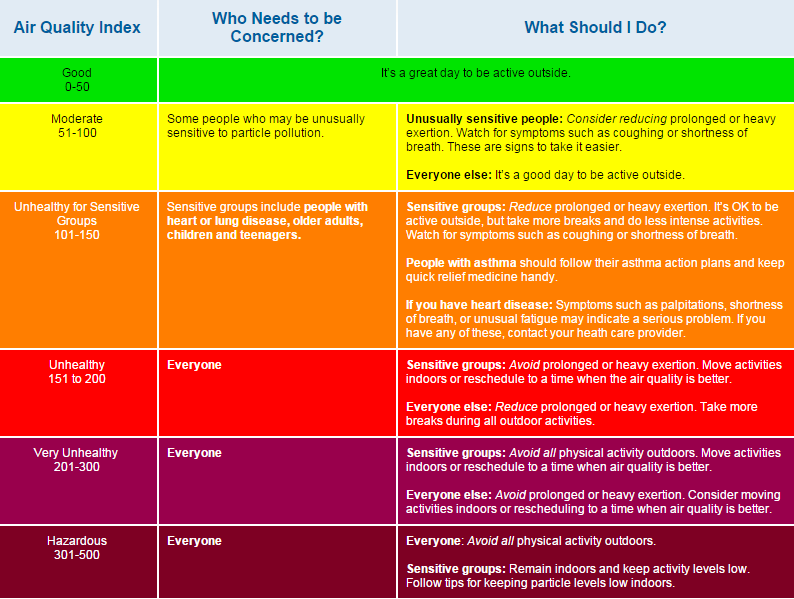
The Air Quality Index is useful because it converts pollutant measurements into a simple warning system. The familiar EPA framework uses six color-coded categories, from green “Good” through yellow, orange, red, purple, and maroon “Hazardous,” with the 2024 AQI update including revised fine particulate matter, or PM2.5, breakpoints.[2] That simplicity is part of the reason patients recognize it. It is also why the AQI can move too easily from public alert to implied clinical intervention.
The clinical question is not whether PM2.5 exposure is harmful. It is. The question is narrower: on a given elevated-AQI day, how many people would need to follow current EPA activity recommendations to prevent one acute cardiopulmonary event? Brook and colleagues put that question into number-needed-to-treat terms in a 2024 JAMA Network Open modeling study, and the resulting estimates are uncomfortable precisely because they translate a familiar warning system into the language of absolute clinical benefit.[3]
What the AQI tells patients, and what it does not
AQI categories are designed to communicate increasing health concern as air pollution rises. At higher categories, public guidance generally shifts from reassurance to reducing prolonged or heavy outdoor exertion, first for sensitive groups and then for broader populations. For many patients, that is a reasonable first screen. A person with severe asthma should not need a randomized trial before being told to take wildfire smoke seriously.
But “reduce outdoor activity” is not one intervention. It can mean skipping a run, moving a walk indoors, staying home from outdoor work if that is economically possible, wearing a respirator, using filtration, closing windows, or doing very little because the patient has no realistic alternative. The AQI category does not by itself specify the achieved reduction in PM2.5 exposure, the patient’s baseline event risk, or the absolute risk reduction expected from a single day of behavior change.
That distinction matters in counseling. A public warning system can be valuable even if it is not a strong individual-level event-prevention tool. A clinical recommendation, however, asks a patient to trade activity, work, access, convenience, or social life for a health benefit. The size of that benefit should be stated with some humility.
The Brook NNT analysis makes the gap visible
Brook et al. modeled the public health relevance of EPA AQI activity recommendations by estimating how many people would need to follow the guidance for one day to prevent one event. The study applied NNT methodology to AQI-based activity advice, using modeled assumptions about PM2.5 exposure reduction and exposure-response relationships rather than direct trial evidence.[3]
The single-day frame is important. These NNTs should not be lined up casually against multi-year NNTs from statin, antihypertensive, or smoking-cessation trials. A one-day behavioral recommendation and a years-long pharmacologic prevention strategy are not the same denominator. Still, when the NNTs move into the millions, the signal is clinically relevant: the expected absolute event reduction from current broad AQI activity advice is very small for most elevated-AQI days.
| AQI condition | Population modeled | Modeled NNT for one day of following guidance | Clinical reading |
|---|---|---|---|
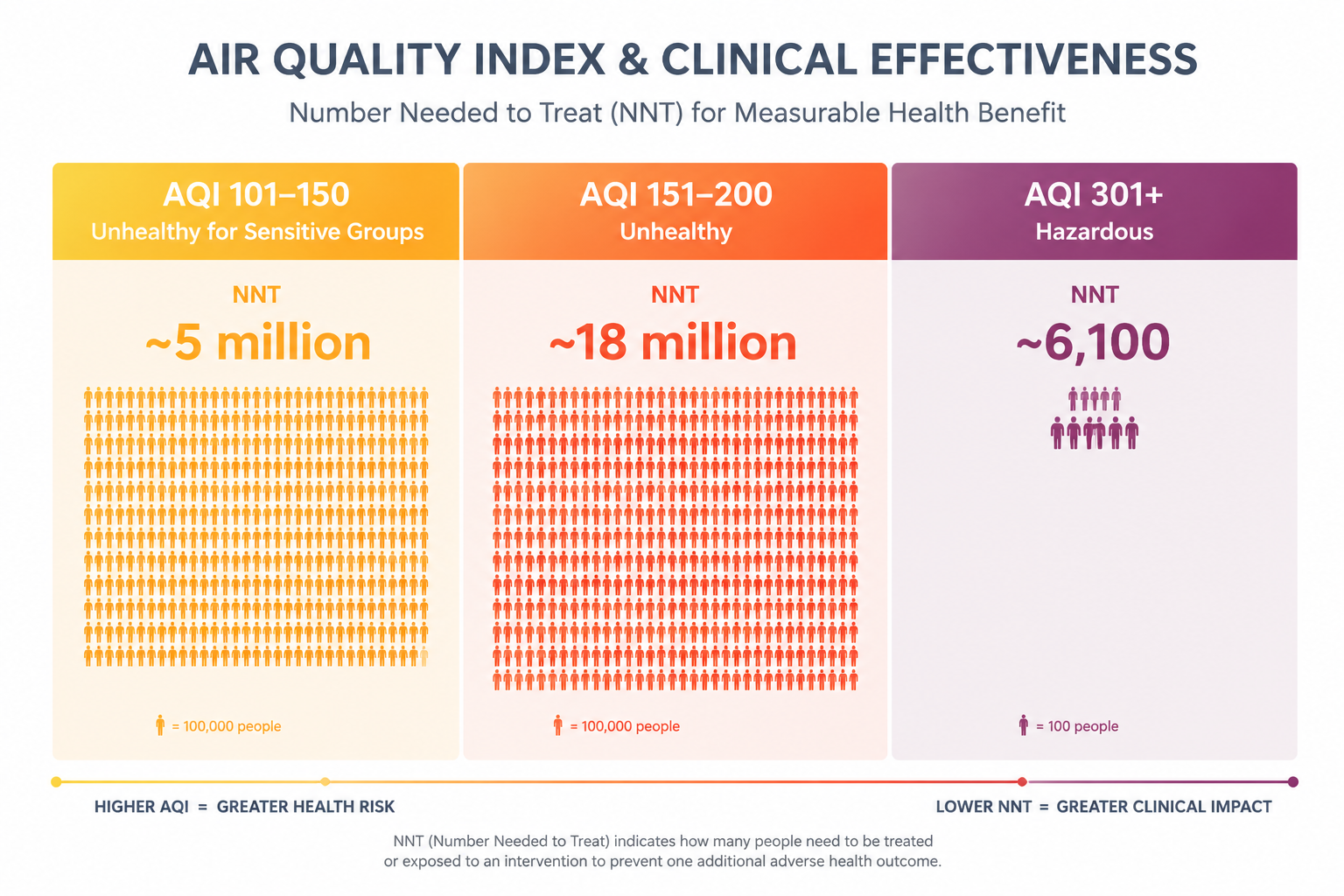
| AQI 101–150 | Patients with ASCVD | Approximately 5 million | Very low absolute cardiovascular event prevention from broad activity guidance.[3] |
| AQI 151–200 | General population | Approximately 18 million | The recommendation reaches more people, but the baseline event risk remains low for most.[3] |
| AQI 151–200 | Patients with ASCVD | Approximately 1.6 million | Risk enrichment improves the estimate, but the NNT remains very large.[3] |
| AQI 301+ | Pulmonary patients | Approximately 6,100 | The estimate begins to look more clinically meaningful, but these Hazardous days represented less than 4% of elevated-AQI days in the analysis.[3] |
The AQI 101–150 range is a good place to see the problem. This is not clean air, and it is not irrelevant for vulnerable patients. Yet the modeled NNT for patients with atherosclerotic cardiovascular disease was approximately 5 million for preventing one cardiovascular event from one day of following the AQI activity recommendation.[3] That number should not be used as a punchline. It should be used as a calibration device.
At AQI 151–200, the current guidance becomes more urgent and applies more broadly. In the model, however, the general-population NNT was approximately 18 million. Among patients with ASCVD, the estimate improved to approximately 1.6 million.[3] That direction makes sense: higher baseline cardiovascular risk should increase the absolute benefit of exposure reduction. But a million-scale single-day NNT remains a difficult basis for strong individual-level cardiovascular event-prevention counseling.
The most clinically persuasive finding appears at the extreme end. During Hazardous conditions, defined as AQI 301 or higher, the modeled NNT for pulmonary patients was approximately 6,100. Those days accounted for less than 4% of elevated-AQI days in the analysis.[3] This is the part of the current AQI framework that feels closest to bedside intuition: when the air is visibly dangerous and pulmonary patients are at immediate risk, protective advice has a more plausible absolute payoff.
That finding should not rescue the entire framework. It supports urgency during rare extreme episodes. It does not show that the more common orange and red categories provide clinically efficient individual cardiovascular prevention when translated into one-day activity restrictions.
Population burden is real; individual absolute benefit can still be small
Air pollution remains a major health hazard at population scale. State of Global Air reported that air pollution contributed to 7.9 million deaths globally in 2023, with 86% of that burden from noncommunicable diseases, predominantly cardiovascular disease.[4] Those figures are not in tension with high NNTs for one-day AQI activity guidance. They are describing different levels of action.
Population-level air quality regulation can shift exposure for millions of people over long periods. A patient-level instruction to reduce outdoor activity on a specific day depends on whether the patient sees the warning, understands it, can change behavior, achieves meaningful exposure reduction, and has enough baseline risk for that reduction to translate into a measurable event difference. A large population burden does not automatically mean that a brief, broad, individual-level activity recommendation has a large absolute benefit for any one patient.
This is where color-coded guidance can mislead without being wrong. Orange and red AQI categories correctly flag worsening exposure. They do not tell a clinician that asking every patient to avoid outdoor activity is a potent preventive intervention for myocardial infarction, stroke, or cardiopulmonary events on that day.
What current clinical counseling can reasonably say
CDC clinical guidance continues to direct clinicians toward using the AQI when counseling patients about air quality and health risk.[5] The American Heart Association scientific statement on personal-level protective actions against particulate matter exposure provides a broader clinical framework for reducing PM exposure, including personal behavior and exposure-reduction strategies.[6] Those materials are still useful in practice, especially when the alternative is silence.
The counseling problem is the implied magnitude. A clinician can tell a patient with COPD to avoid heavy outdoor exertion during smoke without promising that the advice is strongly event-preventive in NNT terms. A patient with ASCVD can be advised to move exercise indoors on poor-air-quality days while also hearing that the strongest cardiovascular protection still comes from sustained risk-factor control, medication adherence when indicated, smoking cessation, and exposure reduction that is feasible over time.
For high-risk patients, the practical message can be specific without being inflated: check the AQI during smoke or pollution episodes; avoid prolonged heavy outdoor exertion when levels are elevated; use cleaner indoor air when available; consider well-fitting respiratory protection when exposure cannot be avoided; and have an action plan for asthma, COPD, or heart failure symptoms. The evidence problem is not that these steps are irrational. It is that broad AQI-triggered activity advice, as currently structured, appears inefficient as single-day event prevention for most people.
Why ASCVD-tailored guidance is the natural next proposal
Brook and colleagues also modeled an alternative approach in JACC Advances: link activity recommendations to estimated 10-year ASCVD risk rather than relying only on AQI category. In that analysis, tailoring restrictions to patients with 10-year ASCVD risk thresholds of at least 7.5%, combined with assumed PM2.5 exposure reductions of 35% to 50%, could lower cardiovascular NNTs below 1 million.[7]
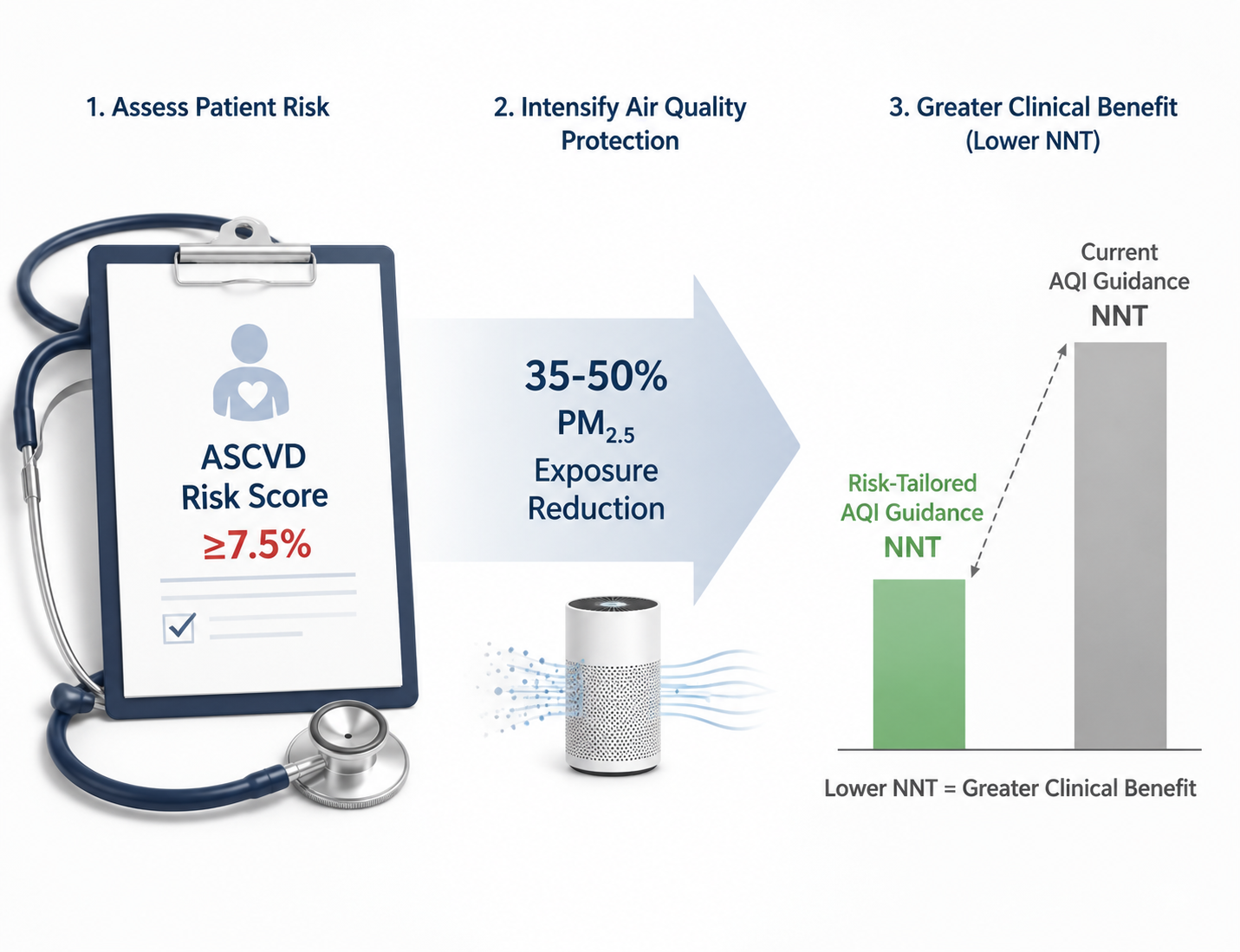
The logic is clinically familiar. If baseline risk is higher, the same relative risk reduction produces a larger absolute risk reduction. If the intervention achieves a larger reduction in PM2.5 exposure, the modeled benefit improves further. The JACC Advances proposal therefore attacks the two weaknesses of broad AQI counseling at once: low average baseline cardiovascular risk in the general population and uncertain exposure reduction from vague activity advice.
Still, “below 1 million” is not the same as clinically robust. The improvement depends on modeled assumptions, including the exposure-response relationship and whether patients can actually achieve a 35% to 50% reduction in PM2.5 exposure.[7] In real life, an office worker with home filtration, an outdoor laborer, a patient in substandard housing, and a person experiencing homelessness do not have the same ability to convert a warning into cleaner air.
Risk tailoring is therefore better understood as a more clinically coherent hypothesis, not a finished recommendation. It gives clinicians a way to prioritize counseling intensity for patients more likely to benefit. It does not turn AQI-triggered activity restriction into a trial-proven cardiovascular prevention strategy.
The assumptions deserve to stay visible
The Brook analyses are models, not randomized trials. That does not make them unimportant. Modeling is often the only feasible way to evaluate environmental exposures and short-term public guidance at scale. But the output is only as credible as the assumptions: the PM2.5 exposure-response function, the degree of exposure reduction achieved by following recommendations, baseline event rates, and the match between AQI category and individual exposure.
The evidence also leaves important uncertainties unresolved. The primary estimates are PM2.5-focused and do not fully account for co-pollutants such as ozone or nitrogen dioxide, which may contribute additional health effects. If personal exposure reduction is less than assumed, real-world NNTs could be higher. If particular high-risk subgroups experience larger exposure-response effects or can achieve larger exposure reductions, their individual benefit could be better than the broad estimates suggest.
The fairest reading is not that AQI guidance is useless. It is that the current category-based activity framework is a blunt instrument when judged as individual-level prevention of acute cardiovascular events. It is more defensible as a public warning system, a trigger for symptom vigilance, and a prompt for especially vulnerable patients to reduce avoidable exposure.
A calibrated clinical position
Poor-air-quality exposure remains a serious cardiopulmonary risk, and the NNT analysis does not weaken the case for population-level air quality regulation. Regulatory action changes exposure distributions over time; one-day individual activity advice works through a much narrower mechanism.
For most elevated AQI days, current EPA activity recommendations appear clinically inefficient as individual-level cardiovascular event prevention, with modeled NNTs in the millions for key cardiovascular outcomes. During rare Hazardous conditions, especially for pulmonary patients, the modeled benefit is more plausible and the protective posture should be stronger. Between those extremes, the counseling should be honest about uncertainty and absolute benefit.
Evidence-minded clinicians do not need to abandon AQI counseling. They need to stop letting the color scale imply more precision than it has. The next version of patient-facing guidance should likely be more risk-tailored, clearer about what behavior is expected to reduce exposure, and explicit that the best-supported estimates for event prevention are modeled rather than trial-proven.
References
- Hazardous AQI Health Risks, The New York Times, July 2026.
- Air Quality Index (AQI) Basics, AirNow.gov.
- Public Health Relevance of US EPA Air Quality Index Activity Recommendations, JAMA Network Open, 2024.
- State of Global Air, State of Global Air.
- How to Use the HeatRisk Tool and Air Quality Index, Centers for Disease Control and Prevention.
- Personal-Level Protective Actions Against Particulate Matter Air Pollution Exposure, Circulation, 2020.
- Enhancing Air Quality Index Activity Guidelines for Preventing Cardiovascular Events, JACC Advances, 2024.
Comments
Join the discussion with an anonymous comment.