The current iceberg lettuce Cyclospora outbreak has a hard number and a soft edge. CDC reported 1,644 confirmed cases, 94 hospitalizations, an age range of 2 to 95 years, a median age of 44 years, and 56% female patients in its July 2026 health alert.[1] Those figures matter, but they are not a clean denominator for illness. In the same advisory, CDC warned that routine stool tests do not always screen for Cyclospora and that clinicians must specifically request diagnostic testing when cyclosporiasis is clinically suspected.[1]
That warning changes how the case count should be read. A patient can have the right exposure window, watery diarrhea, weight loss, cramping, bloating, nausea, fatigue, and a relapsing course, yet never enter the confirmed-case line if the order, specimen collection, staining method, molecular panel, or reporting pathway fails at the wrong point. CDC describes watery diarrhea as nearly universal, with loss of appetite, weight loss, cramping, bloating, nausea, and fatigue among common symptoms; incubation is typically about 1 to 2 weeks, with a range from 2 days to more than 2 weeks.[2]

The outbreak source still matters. FDA traced the 5-state outbreak to iceberg lettuce from Taylor Farms de Mexico served at Taco Bell locations in the affected states.[3] But the diagnostic question comes first because traceback begins after enough illnesses have been recognized, tested, confirmed, and linked. In this outbreak, illness onset was reported from May 1, and CDC issued its health alert on July 14, a gap of more than 10 weeks during which missed or delayed testing could affect both care and surveillance.[1]
The First Failure Point Is the Order
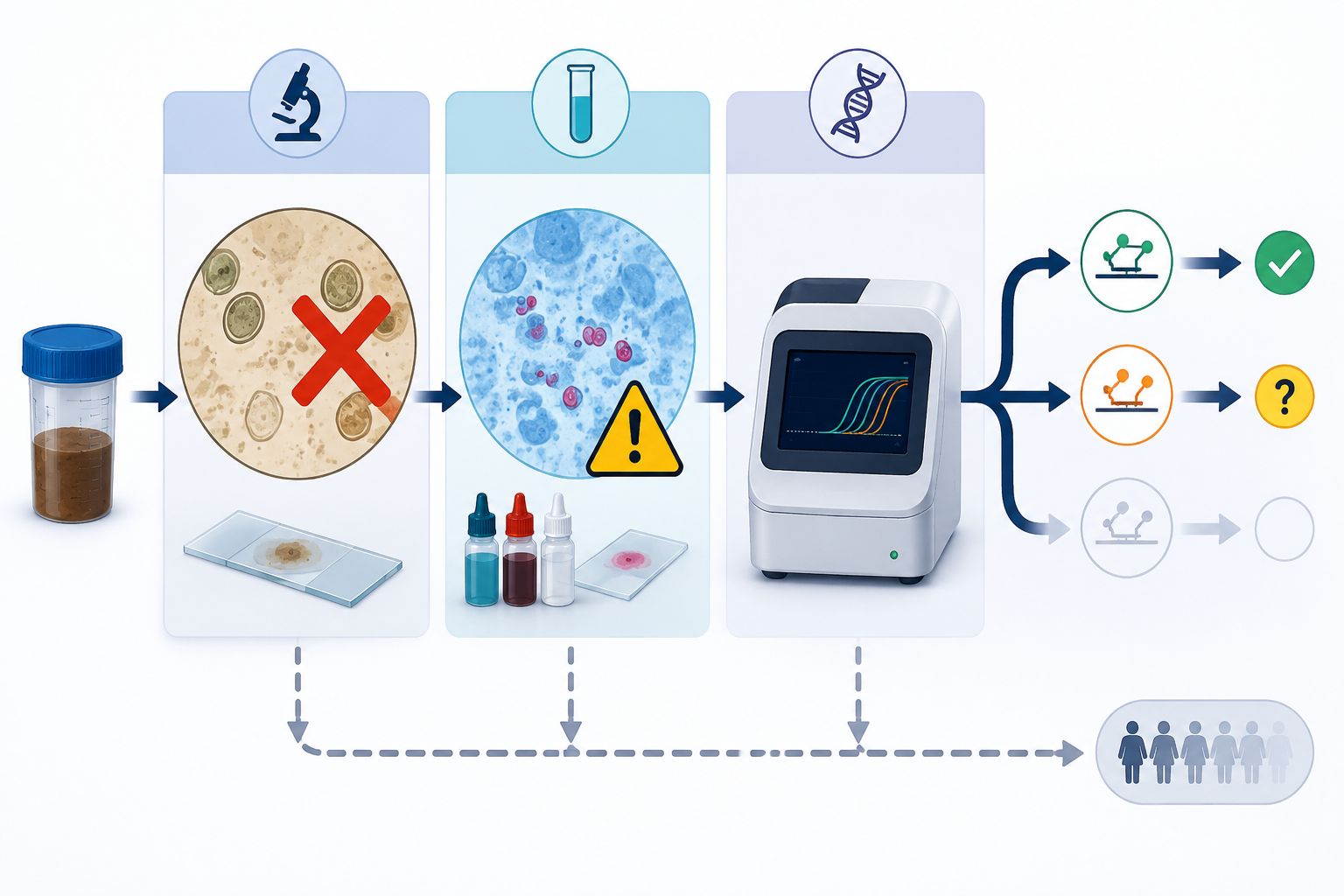
A routine ova-and-parasite order is not the same thing as a Cyclospora workup. The parasite is not reliably detected by standard stool testing unless the laboratory uses an appropriate method and knows to look for it. CDC’s health alert states this plainly: routine stool tests may not include Cyclospora, and clinicians should specifically request testing when symptoms and exposure timing fit.[1]
That is not a minor administrative detail. In many laboratories, an unspecific O&P request can trigger a workflow that is reasonable for common ova and parasites but incomplete for Cyclospora. Modified acid-fast staining may be needed, and it generally requires a specific request. Multiple stool specimens collected on different days can improve the chance of detection, because oocyst shedding may not be captured in a single specimen. Commercial multiplex gastrointestinal panels add another layer of variability: some include Cyclospora targets, and some do not.
| Workflow Point | What Can Happen | Consequence |
|---|---|---|
| Clinical suspicion | Watery diarrhea after a compatible food exposure is treated as nonspecific gastroenteritis | Cyclospora testing is never ordered |
| Routine stool testing | O&P or a GI panel is ordered without confirming Cyclospora coverage | The parasite may not be screened |
| Microscopy | Modified acid-fast staining is not requested or only one specimen is submitted | A true infection can be missed |
| Molecular testing | PCR target and panel design differ across assays | A negative result may depend partly on the assay used |
| Public health linkage | No culture method or PulseNet-equivalent subtyping system is available | Case confirmation and outbreak linkage depend heavily on imperfect detection and epidemiology |
The absence of a culture method matters more than it might appear. For bacterial foodborne outbreaks, culture and molecular subtyping can help connect clinical isolates across places and time. Cyclospora surveillance has no PulseNet-equivalent subtyping system available in routine public health use. That leaves case identification dependent on symptom history, exposure investigation, and tests that may not have been ordered or may not detect the organism.
PCR Is Not One Test
The word PCR can make a result sound settled. For Cyclospora, that confidence needs to be earned assay by assay. A molecular test detects a selected genetic target under a specific extraction, amplification, and interpretation workflow. If two PCR assays look for different targets, they are not interchangeable simply because both are molecular.
Weinreich and colleagues tested this problem directly in a head-to-head comparison of three real-time PCR assays for Cyclospora cayetanensis in 905 stool samples from HIV-positive patients in Ghana. The assays targeted SSU rRNA, 18S rRNA, and hsp70. Agreement among the three assays was only slight, with a kappa of 0.095. Latent class analysis estimated sensitivities of 32.2% for the SSU rRNA assay, 23.3% for the 18S rRNA assay, and 0% for the hsp70 assay.[4]
The least intuitive finding is not merely that sensitivity was low. It is that assays aimed at the same organism did not agree well. When inter-assay agreement is slight, a negative molecular result is no longer a simple statement about whether the parasite is present. It is also a statement about the target selected, the assay chemistry, the specimen, the amount of parasite material in that specimen, and the analytical cutoff used by that laboratory.
The hsp70 result is especially useful as a caution against treating target names as technical trivia. In that study, the hsp70 assay had an LCA-estimated sensitivity of 0%.[4] That does not mean every hsp70-based Cyclospora assay in every laboratory is useless. It does mean that a molecular label alone is not enough. The target and validation context must be visible before the result is allowed to carry clinical weight.
The study population also constrains the claim. The samples came from Ghanaian HIV-positive patients, not immunocompetent U.S. patients in a restaurant-associated iceberg lettuce outbreak.[4] HIV status, geography, background enteric pathogen exposure, stool characteristics, and parasite burden could all affect diagnostic performance. The paper should not be read as a direct U.S. outbreak sensitivity estimate.
But that limitation does not make the comparison irrelevant. The finding that three real-time PCR approaches produced only slight agreement is a method problem as much as a population problem. It tells clinicians and laboratories to ask which assay was used and how it was validated, rather than treating all negative Cyclospora PCR results as equally reassuring.
Microscopy Has Its Own Blind Spots
Modified acid-fast microscopy has a long role in Cyclospora diagnosis, but it is not a rescue from uncertainty. It depends on the organism being present in the submitted specimen, the right stain being performed, and a reader recognizing oocysts that can be difficult to detect. The practical sensitivity problem begins before the slide is read: if the clinician does not request Cyclospora testing, the laboratory may never perform the method most likely to show it.
Repeat specimens matter here because a single stool sample is an imperfect snapshot. For a patient with compatible Cyclospora symptoms after iceberg lettuce exposure, one negative microscopy result should not be given the same interpretive force as a well-timed, repeated, specifically requested evaluation. The more nonspecific the original order, the less meaning a negative result carries.
This is where diagnostic language can mislead. “O&P negative” may mean no ova or parasites were seen under the laboratory’s routine process. It may not mean Cyclospora was specifically sought with an appropriate stain. “GI panel negative” may mean the panel did not include Cyclospora. “PCR negative” may mean one target failed to amplify under one assay’s conditions. These are different negatives, and they should not be collapsed into one clinical conclusion.
Why Confirmed Counts Lag Behind Illness
CDC’s confirmed count is the right number to cite for confirmed cases, but it is not the right number to treat as total infections. The agency noted more than 5,100 additional cases under analysis and stated that the true number of illnesses is likely higher.[1] CIDRAP’s July 17 analysis also emphasized diagnostic delays and the provisional nature of the confirmed count while additional cases remained under review.[5]
That does not justify inventing a multiplier. The evidence supports underascertainment; it does not support a precise estimate of how many infections were missed. Some patients never seek care. Some are seen but not tested. Some are tested with workflows that do not include Cyclospora. Some receive a false-negative result. Some cases remain in state or public health review and have not met the CDC-confirmed case definition.
Case definitions are not bookkeeping trivia. Larger state-level figures, including Michigan’s reported counts, should not be merged with CDC-confirmed numbers as if they used the same numerator. Probable, under-analysis, state-reported, and CDC-confirmed cases answer different questions. Mixing them may make the outbreak look clearer in a headline, but it makes the evidence worse.
The diagnostic lag also affects the clinical story. Untreated cyclosporiasis can last from days to more than a month, and symptoms can remit and relapse.[6] CDC identifies trimethoprim-sulfamethoxazole as the standard treatment regimen, with guidance for patients who have sulfa allergy.[6] Missing the diagnosis therefore is not just a surveillance problem; it can leave a patient with weeks of unexplained watery diarrhea and a clinician cycling through less targeted explanations.
Interpreting a Negative Result During This Outbreak
For clinicians and laboratories, the useful question is not whether Cyclospora testing exists. It is whether the patient’s actual specimen passed through a workflow capable of finding Cyclospora with enough sensitivity to make a negative result meaningful. During an iceberg lettuce outbreak, a patient with watery diarrhea beginning roughly 1 to 2 weeks after a plausible exposure sits in a different pretest-probability category than a patient with brief diarrhea and no exposure history.
- Confirm whether Cyclospora was specifically requested, not merely whether stool testing was ordered.
- Check whether the local GI panel includes Cyclospora and which target it uses.
- Ask whether modified acid-fast staining was performed and whether more than one stool specimen was submitted.
- Interpret a negative result in light of timing, exposure, specimen number, and assay design.
- Separate confirmed public health counts from probable or under-analysis counts when discussing outbreak scale.
The strongest defensible conclusion is narrower than the easiest one to say. The 1,644 confirmed CDC cases likely understate infections, because CDC reports thousands of additional cases under analysis and because routine stool testing may not look for Cyclospora at all.[1] Published head-to-head PCR data show that molecular assays can perform poorly and disagree with each other, but the best available comparison comes from a Ghanaian HIV-positive population and should not be converted into a direct U.S. outbreak sensitivity estimate.[4]
That is enough to change interpretation. In a compatible clinical and exposure setting, an absent routine stool result or a single negative test should not be treated as strong evidence against Cyclospora. The diagnostic system has too many places for the organism to disappear before it becomes a confirmed case.
References
- CDC HAN 00531. Centers for Disease Control and Prevention, July 2026.
- Symptoms of Cyclosporiasis. Centers for Disease Control and Prevention.
- Investigation of 5-State Outbreak of Cyclospora Illnesses: Iceberg Lettuce. U.S. Food and Drug Administration, July 2026.
- Comparison of Three Real-Time PCR Assays for Detection of Cyclospora cayetanensis in Human Stool Samples. Pathogens, 2022.
- What We Truly Know about the Huge US Cyclospora Outbreak — and What We Don’t. CIDRAP, July 17, 2026.
- Clinical Care of Cyclosporiasis. Centers for Disease Control and Prevention.
Comments
Join the discussion with an anonymous comment.