During this cyclosporiasis outbreak, the most dangerous phrase in the chart may be “stool studies negative.” As of July 14, 2026, CDC reported 1,645 confirmed domestically acquired cases across 34 states since May 1, with 141 hospitalizations and no deaths; more than 5,100 additional cases were still under investigation, and the reported age range ran from 2 to 95 years, with a median age of 44 years and 56% female patients.[1] That is already the largest recorded U.S. cyclosporiasis outbreak, but it is not a clean denominator. Michigan had reported 3,309 cases and Ohio 1,119 cases by early July, illustrating how state and federal figures can diverge while investigations are still active.[1][2]
For clinicians, the immediate problem is not whether Cyclospora cayetanensis can cause prolonged illness. It can. The problem is that the organism is easy to miss unless the order tells the laboratory to look for it.

The Clinical Pattern Is Mundane Until It Persists
Cyclospora infection does not usually announce itself in a way that separates it immediately from other causes of gastroenteritis. The incubation period is typically 2 to 14 days, with a median of about 1 week, after ingestion of contaminated food or water.[3] Patients may not connect a salad, prepared produce, restaurant meal, or travel exposure to diarrhea that begins days later.
The syndrome becomes more recognizable with time. CDC describes watery diarrhea as the hallmark symptom, often accompanied by fatigue, loss of appetite, weight loss, bloating, cramping, increased gas, nausea, and low-grade fever; symptoms can last for weeks to months if untreated and may follow a relapsing-remitting course.[3] In practice, that means the patient may improve just enough to cancel follow-up, then return with another stretch of watery stools, exhaustion, and weight loss that no longer fits a simple “stomach bug” timeline.
The 9% hospitalization proportion in the CDC-confirmed 2026 cases should not be read as a marker of high mortality; CDC had reported no deaths as of the July alert.[1] It does, however, separate this illness from the kind of brief, self-limited diarrhea that can safely disappear from clinical attention after hydration advice. A patient who has watery diarrhea for more than a few days, especially with fatigue, weight loss, bloating, or recurrence after partial improvement, deserves a diagnostic plan that includes Cyclospora when exposure timing fits.
Where the Workup Goes Wrong
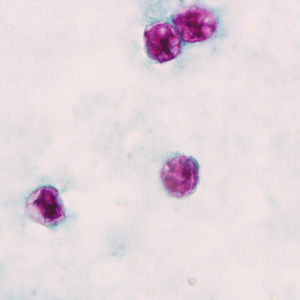
The familiar ova-and-parasite order is not enough. CDC notes that Cyclospora oocysts are small, about 8 to 10 micrometers, and that diagnosis requires specific laboratory testing; the infection is often underdiagnosed and underreported.[4] A routine stool microscopy result that does not include Cyclospora-specific methods can create false reassurance, especially if the report is summarized in the chart as “O&P negative.”
This is the diagnostic bottleneck that matters at the order-entry screen. “Stool testing was done” and “Cyclospora was tested for” are different statements. If a patient has persistent watery diarrhea during a recognized outbreak window, the laboratory request should explicitly ask for Cyclospora detection by a molecular panel that includes it or by a staining method appropriate for the organism.
CDC clinical guidance identifies stool testing by polymerase chain reaction as an option and notes that the BioFire FilmArray Gastrointestinal Panel is FDA-cleared and includes Cyclospora.[5] Reviews of detection methods similarly emphasize that modified acid-fast staining and molecular assays are used because Cyclospora is not reliably found by nonspecific stool examination.[6] The practical implication is simple: if the available gastrointestinal PCR panel does not include Cyclospora, or if the laboratory uses microscopy unless directed otherwise, the clinician has to name the organism.
A Usable Testing Threshold During the 2026 Outbreak
The threshold for Cyclospora-targeted testing should be lower in Q3 2026 than it would be in a quiet season. The CDC alert covers domestically acquired cases beginning May 1 across dozens of states, with thousands of additional reports still under investigation.[1] A patient does not need international travel to fit the outbreak pattern.
| Clinical situation | Order that answers the question |
|---|---|
| Watery diarrhea lasting longer than expected for viral gastroenteritis, especially with fatigue, weight loss, bloating, or recurrence | Stool PCR panel that includes Cyclospora, or Cyclospora-specific PCR if available |
| Persistent watery diarrhea with produce, restaurant, or outbreak exposure and a negative routine O&P | Cyclospora-specific testing; do not treat the prior O&P as exclusionary |
| PCR unavailable or panel does not include Cyclospora | Modified acid-fast staining or another laboratory method specifically validated for Cyclospora detection |
| High clinical suspicion with an initially negative result | Discuss specimen handling, repeat testing, and local public health guidance with the laboratory |
Exposure history still matters, but it should be focused. Ask about fresh produce, prepared salads, restaurant meals, outbreaks reported in the patient’s state, and household or workplace clusters. Do not over-weight a single denied exposure. Foodborne traceback is often more precise after public health investigation than after a patient tries to remember every ingredient eaten 1 to 2 weeks earlier.
The mistake is not ordering stool testing too often. The mistake is ordering a test that cannot answer the clinical question and then allowing the negative result to end the workup. In a patient with compatible symptoms, a negative routine bacterial culture, viral panel, or nonspecific O&P may narrow other causes, but it does not rule out cyclosporiasis unless Cyclospora was actually included.
Treatment Is Specific, Too
CDC recommends trimethoprim-sulfamethoxazole as the treatment of choice for cyclosporiasis: one double-strength tablet, containing TMP 160 mg and SMX 800 mg, twice daily for 7 to 10 days in adults.[5] Pediatric dosing is TMP 5 mg/kg plus SMX 25 mg/kg twice daily for 7 to 10 days.[5] This is another reason the diagnosis matters. Empiric detours with antibiotics that do not treat Cyclospora can prolong illness while adding adverse-effect and resistance concerns.
Sulfonamide allergy is not a small footnote. CDC states that no highly effective alternative therapy has been identified for patients who cannot receive TMP-SMX.[5] Those patients may need individualized management, specialist input, and careful reassessment of the allergy history rather than an automatic substitution that has little evidence behind it.
Supportive care still has a role: hydration, electrolyte assessment when diarrhea is heavy or prolonged, review of immunocompromising conditions, and attention to weight loss. But supportive care should not replace targeted diagnosis when the course, timing, and outbreak context point toward Cyclospora.
Prevention Counseling Has Real Limits
Patients often ask what they should wash differently. The honest answer is narrower than most food-safety scripts. CDC advises washing fruits and vegetables, but also states that washing reduces risk without eliminating it; no EPA-registered disinfectant has been proven effective against Cyclospora on produce, and cooking to at least 158°F (70°C) is the only documented way to kill the parasite.[7]
That does not make produce washing useless. It makes it incomplete. It is reasonable to counsel patients to rinse fresh produce under running water, scrub firm produce, dry it with a clean cloth or paper towel, refrigerate cut produce, and avoid cross-contamination. It is not reasonable to imply that careful household washing can fully control a contamination event that occurred earlier in the supply chain.
The 2026 cluster linked to Taco Bell illustrates the point. CDC reported an outbreak associated with shredded iceberg lettuce served at Taco Bell locations in five states.[8] The lesson is not that an individual patient failed to wash lettuce. The lesson is that traceback, supplier controls, restaurant-level interventions, and timely reporting are the interventions that can stop a distributed exposure.
Why the Counts Should Be Read Cautiously
Confirmed case counts are useful, but they are not the outbreak’s true burden. A case has to become symptomatic, seek care, be tested with the right method, be reported, and then be classified. Cyclospora loses cases at each step. CDC’s own language that cyclosporiasis is often underdiagnosed and underreported should shape how clinicians interpret every total in the 2026 outbreak.[4]
The surveillance context adds more caution. Reported U.S. Cyclospora cases increased from 537 in 2016 to 4,463 in 2023, an 8.3-fold increase over 7 years, according to CDC surveillance data cited in Forbes.[9] Forbes also reported that, starting in 2025, FoodNet made Cyclospora reporting optional for participating states, while the infection remained nationally notifiable in 47 states.[9] Optional reporting does not create disease, but it can affect how quickly a geographically diffuse outbreak becomes visible.
The timing also deserves attention. CDC’s July 14 health alert described cases accumulating since May 1, roughly 10 weeks earlier.[1] That lag does not tell a clinician what caused the outbreak, and it should not be stretched into a conclusion the data do not support. It does reinforce a bedside obligation: when public health signals are delayed or incomplete, diagnosis depends even more on clinicians ordering the right test for the syndrome in front of them.
The Order Has to Say Cyclospora
A practical mental model for this outbreak is short: prolonged watery diarrhea, often after a 1-week incubation; fatigue, bloating, weight loss, and relapse after partial improvement; fresh produce or restaurant exposure that may not be obvious; and a routine stool workup that can miss the diagnosis unless Cyclospora is specified.
In Q3 2026, broad suspicion is not enough. The consequential action is to order Cyclospora-targeted stool testing, by PCR when available or by modified acid-fast staining when needed, for patients whose watery diarrhea has outlasted the usual gastroenteritis script. That is how an individual patient gets treated, and it is also how an outbreak that is already undercounted becomes less invisible.
References
- CDC Health Alert Network (HAN) 00531. Centers for Disease Control and Prevention. July 14, 2026.
- Cyclosporiasis News Release 070826. Ohio Department of Health. July 8, 2026.
- Symptoms of Cyclosporiasis. Centers for Disease Control and Prevention.
- About Cyclosporiasis. Centers for Disease Control and Prevention.
- Clinical Care of Cyclosporiasis. Centers for Disease Control and Prevention.
- Detection Methods for Cyclospora cayetanensis. PubMed Central.
- Preventing Cyclosporiasis. Centers for Disease Control and Prevention.
- Cyclosporiasis Outbreak Linked to Taco Bell. Centers for Disease Control and Prevention. July 2026.
- Unresolved Cyclospora Outbreak Raises Questions Over CDC Cuts. Forbes. July 13, 2026.
Comments
Join the discussion with an anonymous comment.