Lipfendra enters the PCSK9 market with the kind of number that is easy to remember: $315 per month, or $3,780 per year. Against injectable PCSK9 inhibitors that are commonly described in the roughly $500-to-$600 monthly list-price range, the oral drug appears to arrive at a discount of about 40% to 45% before anyone starts discussing rebates, tiers, prior authorization, or coinsurance.[1][2]
That is the visible cost comparison between enlicitide and injectable PCSK9 drugs. It is also the least complete one. Repatha can be purchased through AmgenNow for $239 per month by eligible cash-pay patients, below Lipfendra's list price, while Praluent has been listed through Amazon Pharmacy at $392 per month.[3] Once that counterexample is on the table, the question stops being whether an oral PCSK9 inhibitor has a lower launch list price. The practical question is which doorway the patient, payer, or clinic is using.

The Clean Price Comparison Breaks Quickly
On list price alone, Lipfendra looks disruptive. Repatha and Praluent sit in a higher monthly band, and Leqvio's price is built around an administered, dose-based schedule rather than a conventional monthly pharmacy fill. Inclisiran has been reported at about $3,250 per dose, with twice-yearly maintenance dosing after the initial doses, which makes it relevant to the PCSK9 landscape but awkward as a direct monthly out-of-pocket comparator.[3]
| Therapy | Route and payment feature | Visible price point from available sources | What the number does and does not show |
|---|---|---|---|
| Lipfendra (enlicitide) | Oral daily PCSK9 inhibitor | $315/month; $3,780/year | Launch list price, not yet a net price after rebates or a guarantee of patient cost-sharing |
| Repatha (evolocumab) | Injectable PCSK9 inhibitor | Roughly $500-$600/month list range; $239/month via AmgenNow for eligible cash-pay patients | Cash-pay route can be lower than Lipfendra's list price |
| Praluent (alirocumab) | Injectable PCSK9 inhibitor | Similar list-price range; $392/month listed through Amazon Pharmacy | Cash pharmacy pricing narrows the apparent gap |
| Leqvio (inclisiran) | Administered injectable with dose-based schedule | About $3,250/dose, with twice-yearly maintenance dosing after initial doses | Relevant to injectable PCSK9 economics, but not a clean monthly pharmacy-price comparison |
The table is useful only if it is read as a set of purchasing channels, not as a ranking. A list price can matter for coinsurance and public perception. A cash-pay program can matter for someone without useful insurance coverage. A net price can matter most to the plan deciding tier placement. Those numbers can all describe the same market and still point in different directions.
Cash-Pay Patients May Not See the Oral Drug as the Cheapest Option
For uninsured patients, underinsured patients, or patients whose coverage makes a PCSK9 inhibitor functionally unreachable, the AmgenNow number is the uncomfortable comparator. A $239 monthly Repatha route means Lipfendra's $315 monthly list price is not automatically the lowest patient-facing price in the category.[3]
That does not make the oral option unimportant. It changes the burden of treatment. A tablet avoids injection training, storage concerns, needle aversion, and the small but real workflow involved in starting an injectable. Convenience is not cosmetic when a therapy is intended for long-term risk reduction. But convenience and affordability are separate claims. A patient who can reliably access Repatha at $239 per month has a different cost comparison than a payer staring at undisclosed rebate offers or a Medicare beneficiary facing coinsurance.
Praluent's $392 Amazon Pharmacy listing is different. It sits above Lipfendra's launch list price, but close enough to shrink the headline discount. Once dispensing channel and eligibility rules enter the picture, the gap between oral and injectable therapy becomes less like a single spread and more like a set of exceptions that matter to the person actually paying.[3]
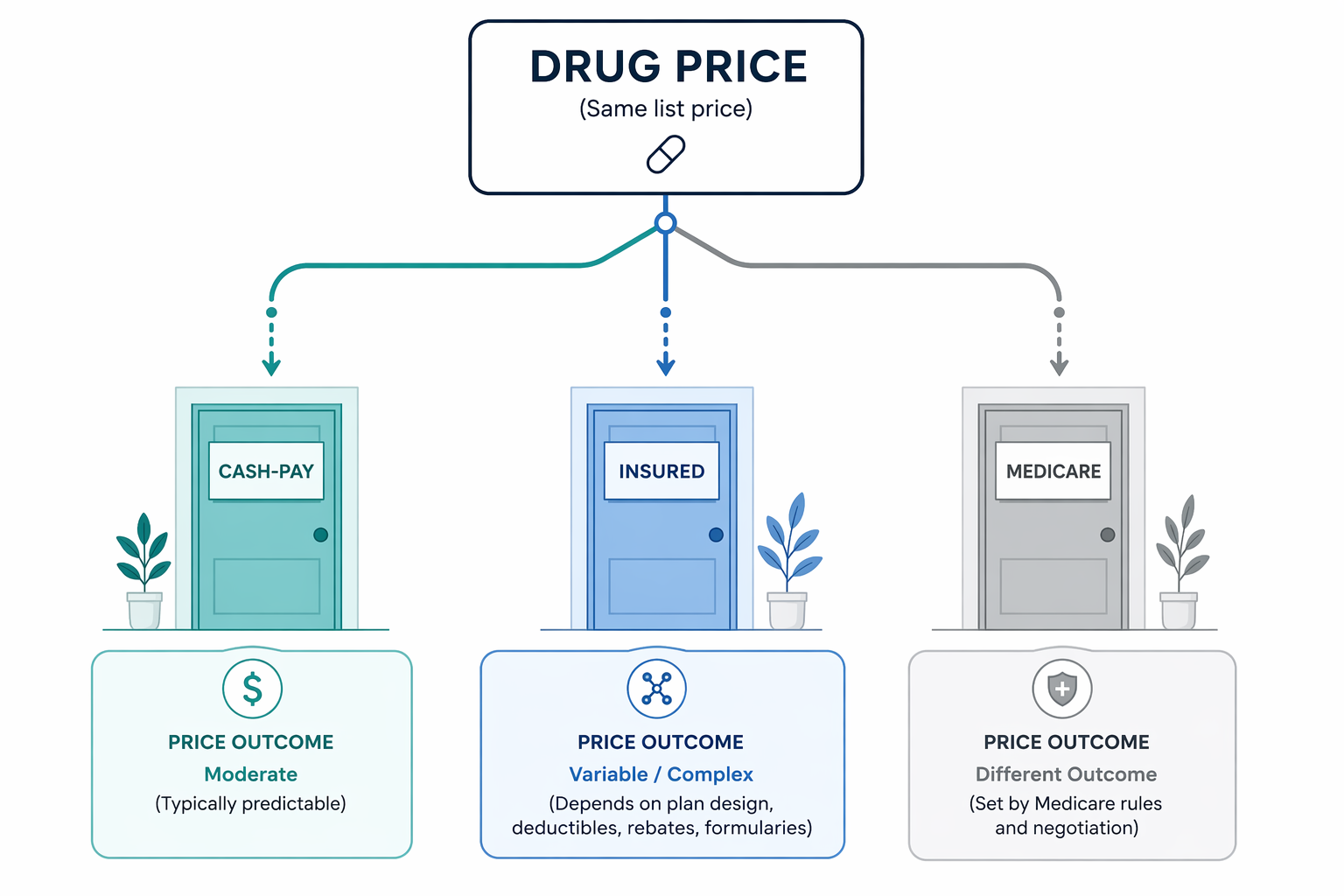
For Insured Patients, the Net Price Is Still Missing
Commercially insured patients rarely experience the list price as a clean bill. Their cost depends on formulary status, tier placement, deductible exposure, copay-card availability, step therapy, and whether the pharmacy benefit treats Lipfendra as preferred, nonpreferred, or blocked pending review. A lower list price gives Merck a useful starting point in negotiations, but it does not reveal the net price a plan or pharmacy benefit manager will actually accept.
That missing net price is not a technical footnote. If injectable competitors defend preferred formulary status with rebates, Lipfendra's visible discount may not translate into lower payer cost. If Merck prices aggressively enough on net and avoids rebate gymnastics, the drug could become attractive for plans that want a less expensive PCSK9 option with an easier route of administration. Both outcomes are plausible from the available information; neither is proven by the launch price.
Medicare is its own problem. Merck has said it aims for broad access, including for the majority of Medicare patients with coinsurance requirements.[4] That statement is worth noting because coinsurance can make list price more visible to patients than a flat copay would. It is not the same as coverage. Until plans publish benefit design, coverage criteria, tiering, and any utilization-management rules, Medicare affordability remains an expectation rather than an observed result.
The Prior-Authorization Bottleneck Has Not Disappeared
The most important economic question may not be whether Lipfendra's list price is lower. It may be whether the patient can get through the same access machinery that has limited PCSK9 use for years. A lower price does not fill out the prior-authorization form, locate the statin history, document ezetimibe use, attach LDL-C values, or answer the denial that comes back because one lab value is too old.
Existing PCSK9 authorization criteria commonly require documentation of maximally tolerated statin therapy or statin intolerance, persistent LDL-C above plan-defined thresholds, and qualifying clinical risk. The thresholds often cluster around LDL-C values of 70 to 100 mg/dL, depending on indication and payer policy.[3] Lipfendra's oral route does not, by itself, remove the payer's incentive to ask the same questions.
That is why the utilization history matters. One analysis described roughly 6 million eligible U.S. adults and estimated that only about 1% were on a PCSK9 inhibitor.[3] The exact figure depends on the eligibility definition, but the direction is hard to ignore: this has not been a category where clinical eligibility smoothly becomes treated prevalence.
For a cardiology clinic, the difference between an injectable and an oral PCSK9 inhibitor may reduce counseling friction. For a pharmacy team, the authorization queue may look familiar. If plans keep requiring the same LDL documentation, statin history, and reauthorization cycle, Lipfendra could be easier to take than injectables without being much easier to start.
Clinical Data Support LDL Lowering, but Outcomes Evidence Is Pending
The clinical case for enlicitide is not thin on LDL-C lowering. In CORALreef Lipids, which enrolled 2,912 participants, enlicitide produced a 56% placebo-adjusted LDL-C reduction at 24 weeks.[5] In CORALreef HeFH, which enrolled 303 adults with heterozygous familial hypercholesterolemia, the placebo-adjusted LDL-C reduction at 24 weeks was 59%.[6]
Those are meaningful lipid results, and they explain why an oral PCSK9 inhibitor immediately attracts attention. They do not answer the payer's outcomes question. Injectable PCSK9 inhibitors have cardiovascular outcomes evidence behind them; enlicitide's outcomes trial is still in progress, with more than 14,500 participants enrolled and results expected around 2029.[5][7]
That timing matters for value assessment. A plan may believe the LDL-C lowering is highly likely to be clinically useful while still reserving broader access until event-reduction data arrive. That is not the same as rejecting the drug. It is the familiar distinction between paying for a biomarker effect and paying for demonstrated reductions in cardiovascular events.
Where Lipfendra Could Still Improve the Economics
Lipfendra's launch price still gives Merck room to change the category. A lower list price can reduce exposure for patients whose cost-sharing is tied directly to list price. It can simplify some employer and plan conversations. It may also make PCSK9 therapy more acceptable to prescribers who have learned, through repeated denials and high pharmacy-counter prices, to hesitate before starting the paperwork.
The oral route also matters operationally. It can remove injection teaching from the clinic workflow and may make the treatment feel less exceptional to patients already taking daily cardiometabolic medications. If Lipfendra receives favorable formulary placement and the authorization criteria are less burdensome than injectables, the practical access improvement could be larger than the list-price discount suggests.
The opposite is also possible. If Lipfendra is placed behind the same prior authorization, faces nonpreferred tiering, or has patient cost-sharing that exceeds available cash-pay injectable options, the oral formulation may improve acceptance without improving affordability. That would leave clinics with a better product experience but a familiar access problem.
The Comparison That Actually Matters
Lipfendra is cheaper than injectable PCSK9 inhibitors in the most visible sense: its $315 monthly list price is below the commonly cited monthly list range for Repatha and Praluent and far below Leqvio's per-dose price.[1][2][3] But list price is only one version of cost. For some cash-pay patients, Repatha's $239 monthly route is lower. For commercially insured patients, undisclosed rebates and formulary decisions will decide the payer's real comparison. For Medicare patients, coinsurance and coverage rules will determine whether Merck's broad-access goal becomes a lower bill.
The fair judgment is narrower than the launch headline. Lipfendra may improve the economics of PCSK9 treatment in some insured and formulary scenarios, and it clearly changes the convenience equation. Its lower list price alone does not establish a broad affordability advantage over injectable PCSK9 drugs. The real comparison will depend on net price, benefit design, cash-pay eligibility, prior-authorization burden, and whether outcomes data eventually make payers more comfortable expanding access.
References
- Merck scores at FDA as Lipfendra becomes world's first oral PCSK9 treatment, Fierce Pharma
- Merck wins first approval of a PCSK9 cholesterol pill, BioPharma Dive
- Lipfendra (enlicitide), the first oral PCSK9 inhibitor, Empirical Health
- Merck press release on Lipfendra approval and access, Merck
- A Placebo-Controlled Trial of the Oral PCSK9 Inhibitor Enlicitide, New England Journal of Medicine
- Efficacy and Safety of Oral PCSK9 Inhibitor Enlicitide in Adults With Heterozygous Familial Hypercholesterolemia, JAMA via PubMed
- FDA Approves Enlicitide, First Oral PCSK9 for High Cholesterol, AJMC
Comments
Join the discussion with an anonymous comment.