A smoke emergency changes the gym-opening question from “indoors or outdoors?” to “how much polluted air will people actually inhale while training?” A facility with HEPA filtration may be a useful cleaner-air option when outdoor running, cycling, or team practice is unsafe. It may also be a poorly measured room where people are moving far more air through their lungs than they would at rest.
That distinction matters for gym access during wildfire smoke health emergencies because exercise changes the dose calculation. During physical activity, minute ventilation can rise roughly 10- to 25-fold, and experimental work by Buonanno and colleagues found that particle deposition may be up to 5 times higher during moderate activity than at rest.[1] The same PM2.5 concentration outside the body is not the same exposure once a person starts intervals, spin class, or a high-repetition lifting circuit.
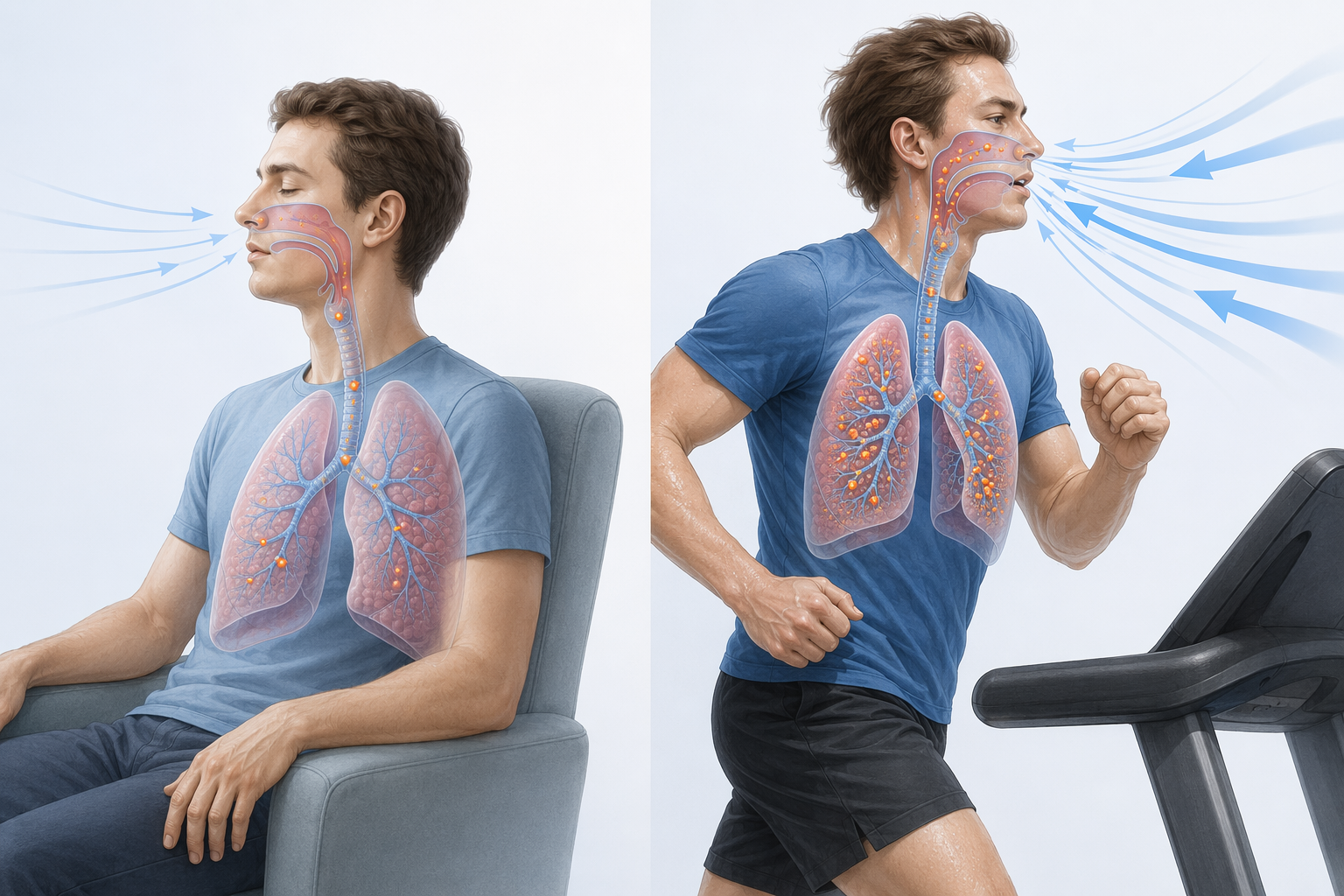
This is why the operational decision cannot stop at whether the building has a roof. A person sitting quietly in a lobby and a person exercising hard in the same room are not receiving the same inhaled dose. The exerciser is pulling more air across airway surfaces, depositing more particles, and doing so at a time when wildfire PM2.5 may already be elevated enough to trigger public health warnings.
The broader cardiovascular context supports caution without answering the facility question by itself. Harvard Chan reporting summarized evidence that a 10-unit increase in PM2.5 is associated with increases in emergency room visits for cardiac events, and described AQI 200 exposure as roughly comparable to smoking about 9 to 10 cigarettes per day.[2] American Heart Association journal evidence also emphasizes cardiovascular risks from wildfire smoke exposure.[3] Those findings explain why smoke is not a mere comfort issue, but they do not tell a manager whether a particular cardio floor is safe enough at 6 p.m.
Filtration Helps, But It Does Not Certify the Room
HEPA filtration deserves to be taken seriously. Extension and EPA-linked guidance on smoke interventions report indoor PM2.5 reductions in the range of 45% to 75% during smoke events when filtration is used effectively.[4][5] In a prolonged wildfire episode, that difference can determine whether people lose access to exercise altogether or have a lower-exposure indoor option.
But filtration performance is not the same as indoor air quality at the point of use. A HEPA unit in one area, an undersized HVAC filter, a door that opens repeatedly to a smoky parking lot, a crowded class, and poor air mixing can produce very different exposures inside the same brand of facility. “We have filtration” is a starting claim. The measured PM2.5 level in the exercise zone is the evidence that should decide what happens next.

The more uncomfortable finding is that gyms are not reliably clean-air spaces even before wildfire smoke enters the discussion. In a 2023 study of 8 health clubs in Portugal, Peixoto and colleagues reported an average PM2.5 concentration of 32.3 µg/m³ and total volatile organic compounds exceeding protective thresholds by 1.6- to 8.9-fold.[6] The study was conducted under post-COVID occupancy limits, so it should not be treated as a direct estimate for every U.S. gym at full capacity. It is still enough to weaken the assumption that a commercial fitness space is low-risk simply because it is indoors.
That matters operationally. Fitness facilities have indoor pollutant sources that offices and homes may not share in the same way: heavy breathing, high occupancy peaks, cleaning products, rubber flooring, equipment materials, and frequent door movement. Ventilation can dilute contaminants, but during wildfire smoke it can also import outdoor PM2.5 unless intake air is filtered well enough. Closing outdoor air dampers may reduce smoke entry in some systems, but it can also worsen CO2, odors, and other indoor contaminants if not managed carefully. The correct setting depends on the building, the system, and the measured room conditions.
The Decision Standard Should Be Measured Indoor Air
A gym that wants to remain open during a wildfire smoke health emergency needs a verification standard, not a reassurance script. The central measurement is indoor PM2.5 in the spaces where people are exercising, not only in a mechanical room, lobby, or manager’s office. A monitor near treadmills may tell a different story than one near the front desk.
| Operational question | Why it matters during smoke | What should be verified |
|---|---|---|
| What is outdoor PM2.5 doing now? | Outdoor smoke sets the pressure on the building envelope and ventilation system. | Current local AQI or PM2.5 from public monitors and nearby sensors. |
| What is indoor PM2.5 in exercise areas? | Exercise multiplies inhaled dose, so the room concentration must be known. | Real-time readings where cardio, group classes, and high-occupancy training occur. |
| Is filtration matched to the room? | A HEPA device can help only if airflow, placement, and maintenance fit the space. | Filter type, clean-air delivery, HVAC settings, filter replacement, and room coverage. |
| How many people are exercising? | Occupancy changes particle generation, CO2, air mixing, and door activity. | Class size, peak-hour density, and whether high-ventilation activities are clustered. |
| Who sees the data? | A hidden reading cannot guide patient counseling or facility decisions. | Visible indoor PM2.5 reporting for staff, clinicians, and members. |
The facility decision then becomes conditional. If outdoor smoke is high but indoor PM2.5 remains low under current occupancy and activity patterns, keeping the gym open may reduce harm for people who would otherwise exercise outdoors or lose a stabilizing health routine. If indoor PM2.5 rises despite filtration, the facility is no longer functioning as a cleaner-air exercise space, even if HEPA equipment is present somewhere in the building.
This also changes the role of the clinician. Counseling a patient to avoid outdoor exertion during smoke is different from advising them that any indoor workout is acceptable. For the outdoor athlete question, the exposure problem is more direct and is covered separately in Why Exercising in Wildfire Smoke Poses Unique Health Risks. For the indoor facility question, the better counseling question is practical: does the gym publish current indoor PM2.5 readings in the areas where you will actually exercise?
What “Open” Should Mean During a Smoke Emergency
A gym can be open in several different ways. It can open all services as usual, limit high-intensity classes, reduce occupancy, shift programming to lower-ventilation activities, make cleaner rooms available for vulnerable members, or close exercise areas while remaining available as a respite space. Those are not equivalent public health choices.
During a smoke emergency, the first defensible threshold is not a single universal class schedule. It is whether the facility can show that indoor PM2.5 is meaningfully lower than outdoor air and remains controlled when people arrive, doors open, HVAC modes change, and classes begin. The harder test is not a reading taken in an empty room at noon; it is a reading during the use pattern the gym intends to permit.
- Keep open with routine programming only when indoor PM2.5 remains low in exercise zones during actual occupancy.
- Modify programming when readings are acceptable at rest but rise during crowded or high-intensity sessions.
- Restrict vulnerable users from high-ventilation workouts when indoor readings are uncertain or fluctuating.
- Close exercise areas when the facility cannot measure indoor PM2.5 or cannot keep it controlled.
- Communicate readings plainly rather than advertising filtration as a substitute for measurement.
EPA wildfire smoke guidance emphasizes reducing exposure, using cleaner indoor air, and adjusting activities during smoke events.[7] For gyms, that guidance should translate into visible indoor monitoring and activity management. A public AQI map may justify concern, but it does not verify the treadmill room.
The measurement problem is also a communication problem. A member deciding whether to attend physical therapy, a group fitness instructor deciding whether to teach, and a cardiology patient trying to preserve a walking routine need more than “we are indoors.” This is where air-quality monitoring and prediction tools may be useful, provided their uncertainty is not hidden. ClinicalMind’s coverage of using AI to improve air quality monitoring for wildfire smoke and AI models for predicting wildfire smoke duration and health effects is most relevant here when these systems help identify when conditions are changing, not when they replace direct indoor measurement.
Why Blanket Closure Is Too Easy
There is a tempting administrative answer: close gyms whenever outdoor AQI reaches a warning level. That may be appropriate when facilities cannot verify indoor air, when smoke infiltrates heavily, or when a community needs simple emergency messaging. But the evidence does not support pretending that every indoor exercise option has the same risk profile.
Brook and colleagues complicate the most rigid version of activity restriction. In JAMA Network Open, they reported that EPA AQI activity recommendations at AQI 101 to 200 had a very high number needed to treat, greater than 18 million for the general population.[8] That finding does not mean smoke is harmless, and it does not address the special inhaled-dose problem of hard exercise in a polluted room. It does warn against treating broad population advisories as if they automatically settle every facility-level decision.
A better rule is less dramatic and more demanding: gym access can be maintained when the facility can demonstrate cleaner indoor air under real operating conditions. That requires functioning filtration, appropriately managed ventilation, occupancy controls when needed, and current PM2.5 readings that members and staff can understand. Without those pieces, the word “indoor” is doing too much work.
A Practical Framework for Facilities and Clinicians
For facility managers, the relevant question is not whether to be pro-exercise or anti-exercise during smoke. It is whether the building is currently reducing exposure for the activities being offered. A gym that wants to remain open should be able to answer, in real time, what indoor PM2.5 is, where it is measured, how filtration is operating, and what will trigger reduced intensity, reduced occupancy, or closure.
For clinicians and medical advisors, the safest counseling language is conditional. Patients who rely on exercise for cardiometabolic health, pain control, rehabilitation, or mental health may need an alternative to outdoor activity during prolonged smoke events. A gym with verified low indoor PM2.5 may be part of that alternative. A gym that cannot provide current indoor readings should be treated as an unknown exposure environment, not as a confirmed safe space.
For public health officials, the message can remain simple without being inaccurate: avoid outdoor exertion during wildfire smoke, prefer cleaner indoor air, and use indoor exercise facilities only when air quality is being measured and controlled. That leaves room for well-run gyms to serve a useful role while removing the unearned safety label from facilities that have not verified their air.
Gyms can plausibly stay open during wildfire smoke health emergencies. They should not stay open on the strength of a filtration claim alone. The defensible standard is measured indoor air quality in the places where people are breathing hardest.
References
- Particle deposition in the human respiratory tract during physical activities, Buonanno et al., 2012
- Harvard Chan School data on wildfire smoke, PM2.5, ER visits, and cigarette-equivalent AQI exposure, Harvard T.H. Chan School of Public Health, 2026
- Cardiovascular risks of wildfire smoke exposure, Circulation Research, American Heart Association, 2024
- Wildfire smoke and indoor air filtration guidance, Oregon State University Extension Service
- Research on DIY air cleaners to reduce wildfire smoke indoors, U.S. Environmental Protection Agency
- Indoor air quality in health clubs, Peixoto et al., 2023
- Wildfire Smoke: A Guide for Public Health Officials, AirNow.gov
- Estimated Health Benefits and Harms of Air Quality Index–Based Physical Activity Recommendations, JAMA Network Open, 2024
Comments
Join the discussion with an anonymous comment.