Two people can receive the same high-pollution alert and make the same sensible choice—stay indoors, reduce exertion, use medication as prescribed—while their bodies do very different things. One may show little measurable change. The other may develop a higher heart rate, faster breathing, more symptoms, or enough concern to contact a clinician. That is the unresolved promise behind AI-driven air quality health advisory recommendations: moving from a citywide warning to an estimate of who is likely to show cardiorespiratory strain today.
The important word is estimate. A model that detects a physiological signal is not yet a system that can tell a patient what to do. The evidence now available suggests that AI can make air quality advisories more physiologically informed before it can make them clinically personal.

What AI-Respire Actually Tested
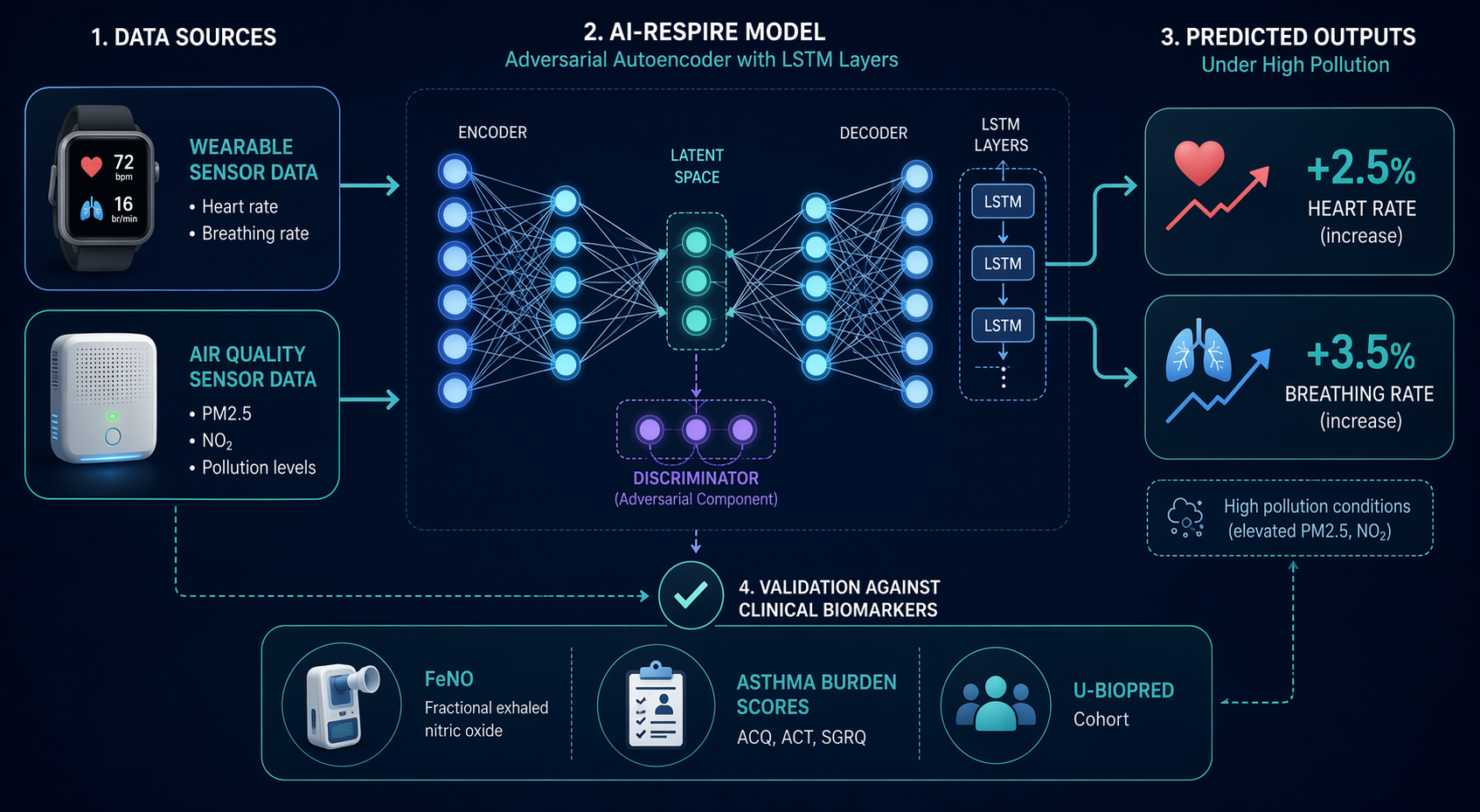
The most relevant evidence comes from AI-Respire, a 2025 Imperial College London framework designed to predict personalized physiological responses to air pollution using wearable and environmental data. Its central claim is not that it diagnoses pollution injury or prevents exacerbations. It is narrower: an adversarial autoencoder model can reconstruct and predict individualized heart rate and breathing rate patterns, then estimate how those signals might shift under simulated increases in pollution exposure.[1]
At a high level, the architecture used an adversarial autoencoder with LSTM and convolutional components. That combination matters because the model was not simply classifying a static risk category. It was trying to learn temporal patterns in physiological data—how breathing rate and heart rate vary over time—while relating those patterns to environmental inputs. The reported reconstruction performance included a mean squared error of 0.0029 for normalized breathing rate reconstruction.[1] That number is meaningful only in context: it describes reconstruction of a normalized signal under the study’s data conditions, not clinical accuracy across devices, diseases, or real pollution episodes.
The study drew on the INHALE dataset, which included 59 participants, but the analysis described in the research brief involved only 10 non-asthmatic participants.[1] That is a small and unusually healthy base for a problem that becomes clinically important precisely in people with asthma, COPD, cardiovascular disease, older age, occupational exposures, or limited ability to avoid polluted environments. The single-user smartwatch fine-tuning is also important: AI-Respire used 8 months of personal smartwatch data from one user for fine-tuning.[1] Longitudinal wearable data are attractive because they can learn a person’s baseline rhythms, but a single-user fine-tuning example cannot establish that the approach transfers across wrist-worn devices, sensor quality, medications, activity levels, or comorbidity profiles.
The most eye-catching result came from simulated pollution increases. AI-Respire examined 20%, 50%, and 100% pollution increase scenarios. Under the simulated 100% increase, the model predicted a 2.5% increase in heart rate and a 3.5% increase in breathing rate.[1] Those are not dramatic numbers, and that is part of why they are worth taking seriously. They sound physiologically plausible rather than theatrical. But they remain model-predicted shifts under simulated exposure conditions, not observed changes during a wildfire smoke day, traffic inversion, industrial episode, or controlled chamber exposure.
| AI-Respire element | What it supports | What it does not yet support |
|---|---|---|
| Adversarial autoencoder with LSTM/convolutional layers | Temporal modeling of wearable physiological patterns | Clinical decision support by itself |
| INHALE analysis of 10 non-asthmatic participants | Early feasibility in a small healthy subset | Generalization to asthma, COPD, cardiovascular disease, or older adults |
| 8 months of single-user smartwatch fine-tuning | Potential value of personal baseline learning | Multi-user, multi-device reliability |
| Simulated 20%, 50%, and 100% pollution increases | A way to stress-test predicted physiological response | Proof of real-world response during measured pollution events |
| Predicted +2.5% heart rate and +3.5% breathing rate under 100% increase | A concrete, plausible cardiorespiratory signal | Evidence that changing behavior based on the alert improves outcomes |
That distinction is the line clinicians will care about. A public-health officer can stand behind a message that says air quality is unhealthy for sensitive groups. A clinician asked to endorse an individualized recommendation needs to know whether the model output means anything for symptoms, medication use, lung function, healthcare utilization, arrhythmia risk, or exacerbation risk. AI-Respire gets closer to the body than a generic AQI band does. It does not yet get all the way to clinical consequence.
Why Heart Rate Is an Interesting Signal, and Why It Is Not Enough
AI-Respire’s clinical bridge used U-BIOPRED, a cohort of approximately 700 participants. In that analysis, elevated resting heart rate was associated with higher asthma burden scores among people with asthma and with elevated fractional exhaled nitric oxide, or FeNO, among healthy volunteers.[1] FeNO is commonly treated as a biomarker related to airway inflammation, so the association gives the heart-rate signal some biological plausibility.
It should not be made to do more work than it can bear. The U-BIOPRED association does not prove that an AI-predicted pollution-induced increase in heart rate causes asthma burden, predicts an exacerbation, or identifies a person who should change medication or cancel activity. It says that elevated resting heart rate was associated with clinically relevant asthma burden measures in one context and with FeNO in healthy volunteers.[1] That is useful because it keeps heart rate from looking like an arbitrary wearable metric. It is insufficient because the clinical question is prospective: if the model alerts this person today, does acting on that alert reduce harm?
Breathing rate has a similar appeal and a similar problem. A breathing-rate shift during pollution exposure may be a plausible marker of respiratory stress, especially if combined with activity, symptoms, medication use, and pollutant levels. But a reconstructed or predicted breathing-rate signal is not automatically a validated respiratory endpoint. Device placement, motion artifact, exercise, anxiety, fever, sleep, and medication effects can all move the same signal. The model may be learning something real without yet learning something actionable.
The Broader AQHI Problem Has Not Been Solved
Personalized models are entering a field whose population-level tools are still methodologically uneven. A 2026 systematic review by Liao and colleagues examined 53 air quality health index studies and found that 66.0% of the articles were published after 2021. Most used single-pollutant approaches: 64.2% were single-pollutant, while 39.6% used multi-pollutant methods. The health outcomes linked to AQHI construction were also varied, with mortality appearing in 56.6% of studies, outpatient visits in 22.6%, and hospitalizations in 13.2%.[2]
Those proportions help explain why the leap to personalized air quality health advisory recommendations is so difficult. The field has not settled on one clean path from pollutant mixture to health outcome even at the population level. If an AI system adds individual wearable data on top of that, it may improve relevance, but it also inherits unresolved choices: which pollutants matter most, whether mixtures are modeled realistically, which outcome the warning is trying to prevent, and whose exposure-response relationship is being represented.
The same review also noted that 88.7% of the AQHI studies were conducted in China.[2] That does not make the evidence weak; it makes its setting visible. Advisory systems are implemented through local pollution mixtures, housing patterns, transport infrastructure, healthcare access, occupational exposures, and public communication norms. A model developed or validated in one environment may not travel well without new calibration and outcome validation.
Risk Mapping Shows What Deployment Might Look Like
A separate 2025 Scientific Reports framework by Rajesh and colleagues shows a different part of the future system: real-time air quality assessment and predictive environmental health risk mapping. The framework used machine-learning methods including Random Forest, Gradient Boosting, XGBoost, and LSTM models; generated 5-minute risk maps; calculated a Health Risk Index normalized from 0 to 1; used SHAP for interpretability; and incorporated demographic overlays for vulnerable populations.[3]
That architecture is useful as a contrast. AI-Respire asks whether one person’s physiology may respond to pollution. Rajesh and colleagues show how an environmental AI system might organize pollutant measurements, maps, risk scores, explanation tools, and vulnerable-population layers into something operationally legible. But the pilot validation used synthetic data with n=100.[3] Synthetic data can help test a pipeline; it cannot establish that the pipeline will behave under sensor failures, sparse monitoring, complex pollutant mixtures, or real clinical vulnerability.
For deployment, these two lines of work would eventually need to meet. A physiologic model without exposure realism risks overpersonalizing a weak environmental estimate. A high-resolution risk map without individual physiology remains closer to conventional public-health alerting. The combination is attractive, but combining two early systems does not make either one validated.
The Alert Message Is Part of the Intervention
Even a technically accurate advisory can fail if people misunderstand it, discount it, or assume it is meant for someone else. In a 2021 controlled experiment with 150 participants, Wu and colleagues found that neutral AQI descriptors lowered risk perception with p<0.001, and that vague target-group language increased third-person perception bias.[4] The study was conducted in China among healthy young adults with a mean age of 29.65, so it should not be treated as a direct proxy for older adults, parents of children with asthma, or patients with cardiopulmonary disease.[4]
Still, the finding lands directly on personalized alerts. If an app tells a user, “Your predicted breathing rate response is elevated today,” the message is not a neutral delivery container. It shapes risk perception and precaution intention. It may reassure, alarm, confuse, or shift responsibility. Communication validation would need to test whether people understand the recommendation, whether they take appropriate precautions, whether high-risk users respond differently from low-risk users, and whether clinicians can explain the alert without reverse-engineering the model.
This is where a model’s apparent precision can become a liability. A citywide advisory is blunt, but its bluntness is visible. A personalized score can look more certain than it is, especially when presented beside heart-rate curves, breathing-rate changes, or risk colors. If the evidence behind the score comes from 10 non-asthmatic participants, simulated exposure increases, and single-user fine-tuning, the user interface has to preserve uncertainty rather than polish it away.
Personalization Cannot Substitute for Exposure Reduction
There is also a population-level risk in making pollution advice too individual. Ambient pollution harms are not evenly distributed, and the people most exposed are not always the people with the most freedom to respond. The American Heart Association’s 2020 policy statement reported that, per 10 μg/m³ increase in PM2.5, Black populations had a hazard ratio of 1.21 compared with 1.06 for White populations. It also noted that 132 million people lived in counties not compliant with air quality standards and that 17,000 U.S. schools were within 250 meters of high-traffic roads.[5]
Those facts matter because a personalized advisory often tells the recipient to adapt: avoid outdoor exertion, change timing, filter indoor air, or seek care if symptoms worsen. Some people can do those things. Others work outdoors, commute through high-traffic corridors, attend schools near roads, live in poorly sealed housing, or cannot afford filtration. A model that predicts individual strain may help identify need, but it does not remove the exposure that created the need.
The AI infrastructure itself also has a pollution footprint. A 2026 Harvard Chan School analysis reported that one AI data center gas plant in Virginia could be associated with $53 million to $99 million in annual health damages, 3.4 to 6.5 additional premature deaths per year, and disproportionate impact on communities with high social vulnerability.[6] That example does not mean AI should be excluded from environmental health. It means the health accounting cannot stop at the app screen.
What Would Make the Evidence Clinically Stronger
The missing evidence is not mysterious. For personalized air quality health advisory recommendations to move from research direction to clinical deployment, the next studies would need to observe real exposure events rather than only simulate pollution increases. They would need enough participants to evaluate performance across asthma, COPD, cardiovascular disease, age groups, medications, pregnancy status where relevant, occupational exposure, and baseline fitness. They would need multiple wearable devices and transparent handling of missing or noisy data.
They would also need outcome linkage. A predicted 2.5% heart-rate increase is not a clinical endpoint. A stronger study would ask whether the predicted response is associated prospectively with symptoms, rescue medication use, peak flow or spirometry changes when available, FeNO shifts, arrhythmia events where relevant, urgent visits, missed school or work, or patient-reported functional limitation. The outcome does not have to be hospitalization for the model to matter, but it has to matter outside the model.
Finally, recommendation studies would need to test the advisory itself. A system could be accurate and still unhelpful if it prompts too many false alarms, shifts activity away from beneficial exercise without reducing exposure, increases anxiety, or gives low-risk reassurance to someone whose symptoms require care. The safest near-term role may be decision support for public-health research and physiologic risk stratification, not autonomous advice to patients.
Readiness in Q3 2026
By Q3 2026, the evidence supports cautious enthusiasm for AI that makes air quality advisories more physiologically informed. AI-Respire shows that wearable and environmental data can be modeled together, that individual heart rate and breathing rate responses can be predicted under simulated pollution increases, and that heart-rate signals have some clinical plausibility through associations with asthma burden and FeNO.[1]
The evidence does not yet support clinical deployment of personalized air quality health advisory recommendations or individual clinical decision support. The core framework remains limited by a small non-asthmatic analyzed cohort, single-user smartwatch fine-tuning, simulated exposure scenarios, uncertain generalizability to high-risk groups, and no prospective evidence that AI-generated personalized recommendations improve health outcomes. The research direction is real. The clinical advisory is not ready to stand on its own.
References
- An AI-driven framework for the prediction of personalised health response to air pollution. Imperial College London. 2025.
- Developing air quality health index: A systematic review of concepts and approaches. Hygiene and Environmental Health Advances. 2026.
- Machine learning-driven framework for realtime air quality assessment and predictive environmental health risk mapping. Scientific Reports. 2025.
- Communicating Air Quality Index Information: Effects of Different Styles on Individuals' Risk Perception and Precaution Intention. 2021.
- Guidance to Reduce the Cardiovascular Burden of Ambient Air Pollutants. Circulation. 2020.
- Analyzing air pollution health, economic risks from AI data centers. Harvard Chan School. 2026.
Comments
Join the discussion with an anonymous comment.