By midday on July 17, Richmond’s smoke problem had already stopped being a visibility problem and become an operations problem. The city reached Code Purple, the second-worst air quality designation, while more than 130 million Americans were under air quality alerts. Richmond Ambulance Authority reported that calls for breathing problems and chest pain had already reached what the agency would normally expect across a full 24-hour day.[1]
That is the part of the July 2026 smoke event that should stay with hospital and public health planners. A bad AQI forecast is abstract until the EMS queue starts filling before lunch. The causes of smoky air health effects in Richmond were not mysterious, but the speed of the clinical load matters: transported wildfire smoke can turn a regional air alert into a local respiratory and cardiovascular surge within hours.

Local agencies and clinicians were already trying to translate the alert into practical behavior before Richmond hit Code Purple. Virginia DEQ, VCU Children’s Hospital, and local pulmonologist Dr. John Sentz issued real-time guidance as smoke conditions worsened, with attention to children, people with asthma or chronic lung disease, and those who could not easily avoid outdoor exposure.[2] For administrators, the same guidance has a second function: it identifies where demand is likely to appear first. Pediatric practices field calls. Pulmonology offices adjust advice. ED triage sees anxious breathing, wheeze, chest tightness, and exacerbations that may have started hours earlier at home.
Why wildfire smoke moves so quickly from air alert to clinical demand
The relevant exposure is not simply “smoke.” The operational concern is fine particulate matter, especially PM2.5, small enough to penetrate deep into the lungs. CDC describes wildfire smoke as a mixture of gases and fine particles that can irritate the respiratory tract, worsen asthma and chronic obstructive pulmonary disease, and contribute to heart-related symptoms in susceptible people.[3]
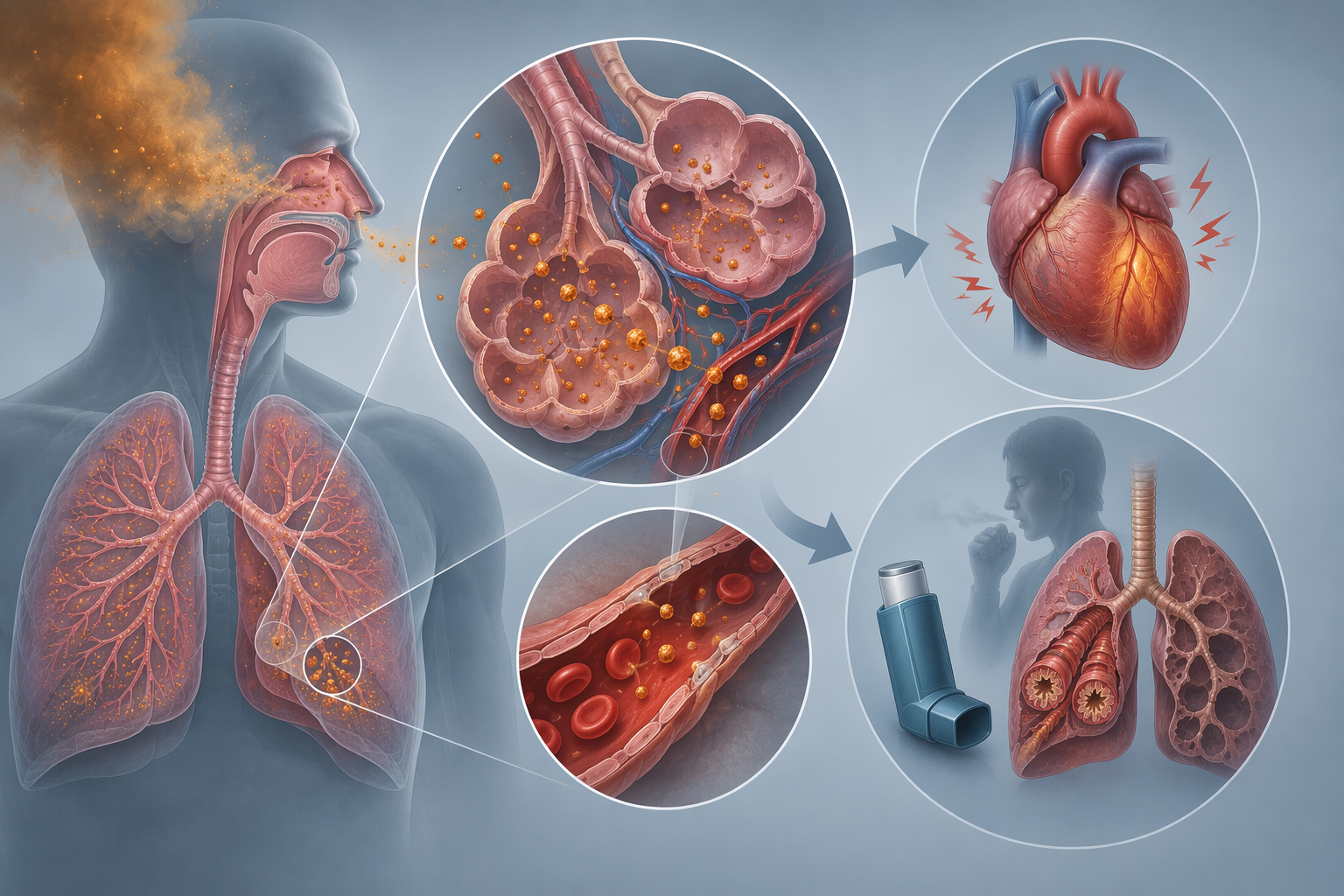
That mechanism explains why the EMS signal in Richmond was not confined to obvious respiratory complaints. PM2.5 exposure can aggravate airway inflammation and bronchoconstriction, but it can also increase cardiopulmonary strain. For a dispatcher or charge nurse, the important distinction is that smoke days do not present as one clean category. Asthma exacerbations, COPD flares, shortness of breath, chest pain, dizziness, and anxiety about breathing can all arrive through different doors while the source exposure is shared.
The asthma evidence is particularly useful because it connects a measured pollutant increase to ED demand. In one cited study, each 10 µg/m³ increase in wildfire PM2.5 was associated with an 11% increase in asthma emergency department visits.[4] Another analysis found fire-related PM2.5 had a relative risk of 1.46 for asthma ED visits, compared with 0.77 for non-fire PM2.5.[5] Those numbers should not be stretched into a Richmond-specific prediction, but they do support the basic clinical plausibility of what EMS saw: wildfire particles can produce more than a nuisance-level increase in acute respiratory utilization.
Children sit high on the concern list because they breathe more air relative to body size and may have less reserve when asthma or viral-season vulnerability overlaps with smoke exposure. Older adults and patients with established asthma, COPD, heart disease, or occupational outdoor exposure are also more likely to convert the same AQI alert into a clinical encounter. In surge planning terms, the problem is not only how toxic the air is. It is how many people with limited physiologic margin are exposed at the same time.
Richmond was not starting from a clean baseline
The July 2026 Code Purple episode landed in a city whose particle pollution profile was already worsening. The American Lung Association’s 2025 State of the Air report gave Richmond a C for daily particle pollution, down from a B, and ranked the city 98th worst nationally for that measure.[6] That grade is not a disaster plan by itself. It is a warning that a transported-smoke day is arriving on top of a local baseline that already deserves attention.
The regional planning horizon is also shifting. First Street Foundation projections reported through Axios Richmond indicated that more than half of Virginia — 75 localities — will see increased bad-air-quality days over the next 30 years.[7] For a Mid-Atlantic health system, that moves wildfire smoke out of the category of rare Western disaster footage and into the same planning conversation as heat, respiratory virus season, and EMS diversion pressure.
National exposure data point in the same direction. Stanford ECHO Lab analysis reported by Climate Central found that per-person U.S. wildfire smoke exposure was four times higher during 2020–2024 than during 2006–2019.[8] A 2025 Nature study estimated that wildfire smoke caused about 164,000 premature deaths in the United States from 2006 to 2020, with about 15,000 attributable to climate change.[9] Those figures are too broad to tell Richmond how many ambulances to stage. They do, however, make it harder to treat a Code Purple day as an isolated anomaly.
The missing interval is not the alert; it is the usable lead time
Most public-facing smoke guidance begins when the air is already bad or forecast to become bad soon. That is useful for individuals deciding whether to go outside, and it matters for schools, outdoor workers, clinics, and long-term care facilities. But a hospital or EMS agency needs a different clock. Respiratory staffing, bronchodilator inventory checks, clinic messaging, call center scripts, EMS coordination, and high-risk patient outreach all become easier if the signal arrives before the morning dashboard turns purple.
This is where AI and machine learning forecasting becomes interesting, not because the terminology is impressive, but because the timing could change decisions. CIRES and NOAA presented an AI-driven subseasonal-to-seasonal wildfire emissions forecasting system in January 2026 that aims to predict wildfire emissions 35 to 45 days ahead by combining seven global fire emission inventories with meteorological and land-use data.[10] That is not the same thing as a clinically validated Richmond smoke-surge forecast. It is an upstream capability: a way to estimate when fire emissions may become more likely before smoke transport, local meteorology, exposure patterns, and health system demand are fully known.
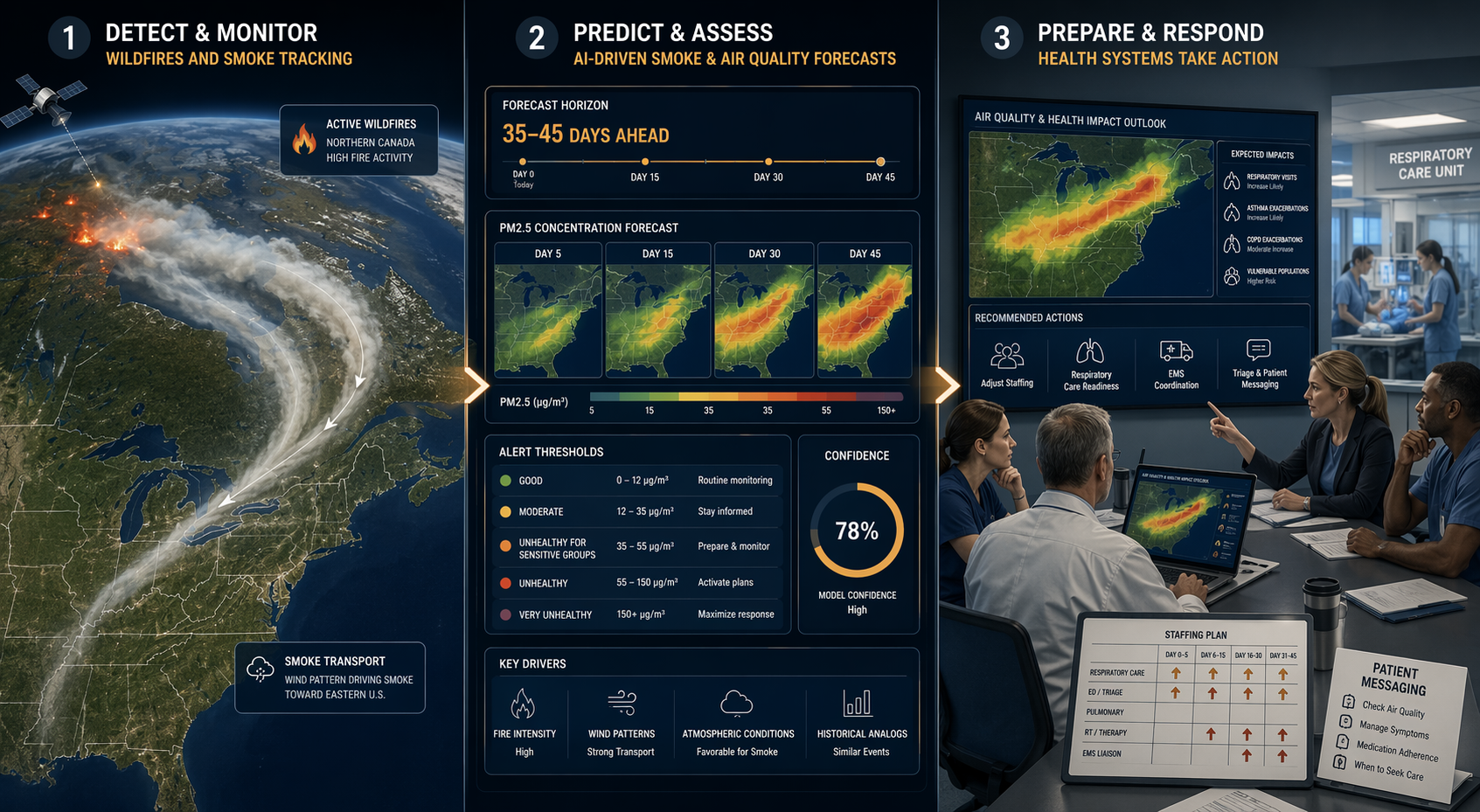
The practical question is what a planner would do differently with that signal. A 35- to 45-day emissions outlook could support scenario planning: review respiratory therapist coverage, identify clinics serving high-asthma-burden neighborhoods, prepare school and pediatric messaging templates, and ask EMS partners how they would handle a same-day rise in breathing and chest-pain calls. A shorter-range local PM2.5 forecast could trigger more concrete actions: adjust triage language, pre-position phone advice, warn outpatient practices, and coordinate public messaging before avoidable exposure peaks.
Different model types sit at different points in that chain. The CIRES/NOAA system addresses emissions risk weeks ahead.[10] Random Forest approaches have been reported to estimate PM2.5 exposure with accuracy as high as 98.2%, a monitoring and exposure-estimation function rather than direct proof of clinical outcome improvement.[11] BlueSky, used in British Columbia, linked predicted PM2.5 increases with actual upticks in bronchodilator prescriptions, giving a more operationally relevant example of forecasted smoke aligning with medication demand.[12]
| Forecast capability | What it can help a health system do | What it does not prove by itself |
|---|---|---|
| Weeks-ahead wildfire emissions signal | Start staffing scenarios, agency coordination, and high-risk patient communication planning | That Richmond-level PM2.5 or EMS demand will occur |
| Local PM2.5 exposure estimation | Identify where exposure is likely to be highest and compare neighborhood risk patterns | That a specific intervention reduced ED visits |
| Smoke forecast linked to medication demand | Prepare pharmacies, clinics, and respiratory teams for likely increases in bronchodilator use | That every region will show the same relationship |
What validation has to look like for Eastern smoke events
The hard part for Richmond is not believing that smoke can travel. The hard part is validating a forecast chain across emissions, transport, local PM2.5, exposure, symptoms, and operational demand. A model may be good at estimating pollution concentration and still be poor at predicting when EMS calls will spike. A system may work well in a region with frequent wildfire smoke experience and still need testing for Mid-Atlantic episodes driven by long-range transport.
The 2026 review by Ye and colleagues is helpful here because it frames machine learning as an emerging frontier in wildfire-health research, not as a finished clinical product. The review covered 139 studies and noted that machine learning approaches accelerated notably after 2021.[11] That growth matters, but adoption of a method is not evidence that it improves patient outcomes or prevents surge. For hospital use, the needed endpoint is not only forecast accuracy. It is whether the forecast changes a decision early enough to matter.
A useful Richmond validation study would not stop at comparing predicted and observed AQI. It would ask whether the model anticipated local PM2.5 timing, whether alerts reached health system users with enough lead time, whether EMS and ED respiratory and chest-pain volumes rose as expected, and whether pre-planned actions reduced bottlenecks. It would also separate vulnerable groups rather than averaging them away: children with asthma, adults with COPD, older patients with cardiac disease, outdoor workers, and patients with limited access to filtered indoor air.
This is also where risk communication can fail. A purple AQI category tells the public that conditions are dangerous, but it does not automatically tell a pediatric clinic when to message families, an EMS supervisor when to expect call concentration, or an ED charge nurse whether to hold an extra respiratory therapist. AI-assisted dashboards will not solve that by adding another color scale. They need to map forecasts to pre-agreed actions.
Preparedness decisions that could move upstream
If a credible smoke signal appears days to weeks ahead, the first useful response is not alarm. It is assignment. Someone has to own the forecast, decide whether it meets an action threshold, and translate it into work orders, staffing options, and public-facing language. Without that chain, a model output becomes one more dashboard watched by people who are already busy.
- EMS can compare forecast windows with staffing, special events, heat risk, and diversion patterns.
- ED leaders can decide when respiratory therapy backup, triage scripts, and fast-track pathways need review.
- Pulmonology and primary care clinics can prepare advice for asthma and COPD patients before phone volume rises.
- Pediatric teams can coordinate messaging with schools, camps, and caregivers of children with known respiratory disease.
- Public health agencies can align AQI language with concrete local actions instead of issuing generic stay-inside reminders.
None of those actions requires pretending the forecast is perfect. They require knowing which decisions are low-regret and reversible. Drafting clinic messages, reviewing respiratory staffing contingencies, and coordinating EMS communication are different from canceling services or declaring an emergency. The threshold for preparation can be lower than the threshold for disruptive action.
Richmond’s July 2026 event makes the distinction visible. By the time breathing-problem and chest-pain calls had reached a normal full-day volume at midday, the system was already absorbing the surge.[1] Forecasting is valuable only if it shifts some of that work earlier: not by promising that AI will prevent symptoms, but by giving local teams a better chance to prepare for the moment when the air quality category becomes a staffing, triage, and EMS problem.
Richmond keeps the conclusion narrow. Smoky air health effects were driven by wildfire PM2.5 exposure that can aggravate respiratory disease, stress the cardiovascular system, and concentrate demand among vulnerable patients. AI and machine learning systems may help move response upstream, especially when emissions forecasts, PM2.5 exposure models, and health-utilization signals are connected. Before local agencies rely on them for major operational decisions, they need validation for transported Eastern U.S. smoke events, integration into clinical workflows, and action thresholds that administrators can use before the AQI turns purple.
References
- Richmond hits Code Purple as wildfire smoke blankets area, WTVR CBS 6, July 17, 2026.
- Experts weigh in on air quality alert, 12 On Your Side / WTVR, July 16, 2026.
- How Wildfire Smoke Affects Your Body, CDC.
- Clearing the Air: Wildfire Smoke and Asthma/COPD, PMC, 2024.
- Association of Wildfire Air Pollution and Health Care Use for Atopic Dermatitis and Itch, Malig et al., 2021.
- State of the Air, American Lung Association, April 2025.
- Virginia air quality projections, First Street Foundation via Axios Richmond, March 2024.
- Climate Change Worsens Wildfire Smoke, Climate Central, 2025.
- Wildfire smoke deaths in the United States from 2006 to 2020, Law et al., Nature, 2025.
- AI takes on wildfire emissions forecasting, CIRES/NOAA, January 2026.
- Wildfires and Public Health: Comprehensive Review, Ye et al., PMC, 2026.
- BlueSky smoke forecast system and bronchodilator prescription changes, Yao et al., 2013.
Comments
Join the discussion with an anonymous comment.