Wildfire smoke health risks and AI monitoring now sit in an uncomfortable place: the exposure problem is already a public-health burden, while the monitoring tools are becoming operational faster than their health benefits have been proven. Wildfire PM2.5 has been reported as roughly 10 times more toxic per unit mass than fossil-fuel PM2.5, with no safe exposure threshold identified in the Stanford work summarized in 2025.[1] Long-term wildfire PM2.5 exposure has also been associated with about 11,415 non-accidental deaths each year in the contiguous United States, according to Yale coverage of a PNAS study.[2]
Those numbers explain why a smoke dashboard cannot be judged only by whether it draws a sharper plume. The practical question is whether an alert reaches the people who can close schools, staff clinics, protect outdoor workers, warn high-risk patients, or change hospital operations before the smoke becomes obvious. A technically strong model that stops at “alert issued” still leaves the hardest part of the public-health response chain unfinished.

The mismatch becomes clearer in urban fires. Smoke from burned buildings, vehicles, plastics, household goods, and infrastructure can carry hazards that ordinary particulate summaries do not describe well. Reporting on urban wildfire smoke has highlighted lead, chlorine, and benzene at 40 to 110 times normal levels, and noted that standard AQI does not capture that chemical detail.[3] For a health department or hospital planner, “PM2.5 is high” and “the plume may contain toxic combustion products from an urban burn” are not the same operational message.
Where AI Is Strongest: Finding Fire Early
The cleanest evidence in the AI wildfire smoke monitoring pipeline is early detection. Computer vision and edge AI systems can identify ignitions within 5 to 10 minutes, with reported detection accuracy of 95% to 98% and false-alarm rates below 2%, according to the U.S. Government Accountability Office’s 2025 review.[4] In emergency operations terms, that is not a vague promise. It is a time window someone can build around.
Five to 10 minutes after ignition does not automatically mean five to 10 minutes of health protection. It can mean faster verification, earlier dispatch, earlier plume modeling, and earlier notice to air quality and public-health staff. Whether it changes evacuation timing, school decisions, medication guidance, or clinical surge planning depends on the chain that follows. Still, among the stages of the pipeline, detection has crossed furthest from demonstration into operational usefulness.
GAO also notes barriers that matter for deployment rather than model publicity: high up-front data preparation costs and limited historical data for rare extreme events.[4] That caveat should not erase the detection performance. It should keep agencies from assuming that a tool proven in one camera network, terrain, fuel type, or weather context will behave identically everywhere.
Forecasting Smoke Is Harder Than Detecting Ignition
Once a fire is detected, the next question is where smoke will go, how concentrated it will become, and how long communities will be exposed. This is where AI begins to share the stage with atmospheric chemistry, emissions estimation, weather, terrain, and human activity. Hybrid models are attractive because they do not ask machine learning to replace physical modeling; they use machine learning to improve pieces of a system that still needs chemical transport logic.
One reported comparison found that hybrid machine-learning and chemical-transport approaches outperformed either method alone by 66% and 12%, respectively.[5] The important point is not that AI “wins” against traditional models. It is that smoke forecasting appears to improve when statistical learning and physical constraints are used together, especially for a pollutant mixture that moves across jurisdictional boundaries faster than many public-health approval processes.
Longer lead time is the tempting prize. CIRES and NOAA reported in January 2026 that an AI emissions prediction system can forecast wildfire emissions 35 to 45 days ahead.[6] For hospitals, school districts, air agencies, and public-health departments, a credible sub-seasonal signal could support staffing plans, respirator distribution, clean-air shelter planning, public messaging, and coordination with long-term care facilities before an acute smoke episode arrives.
But a 35- to 45-day forecast is not a clinical warning order. The same report flags limited skill during extreme wildfire seasons.[6] That distinction matters. A forecast can be useful for preparedness even when it is not reliable enough for a specific patient-level intervention or a school closure decision. Treating every extended smoke forecast as certainty would move the error downstream to exactly the people who must defend the decision in public.
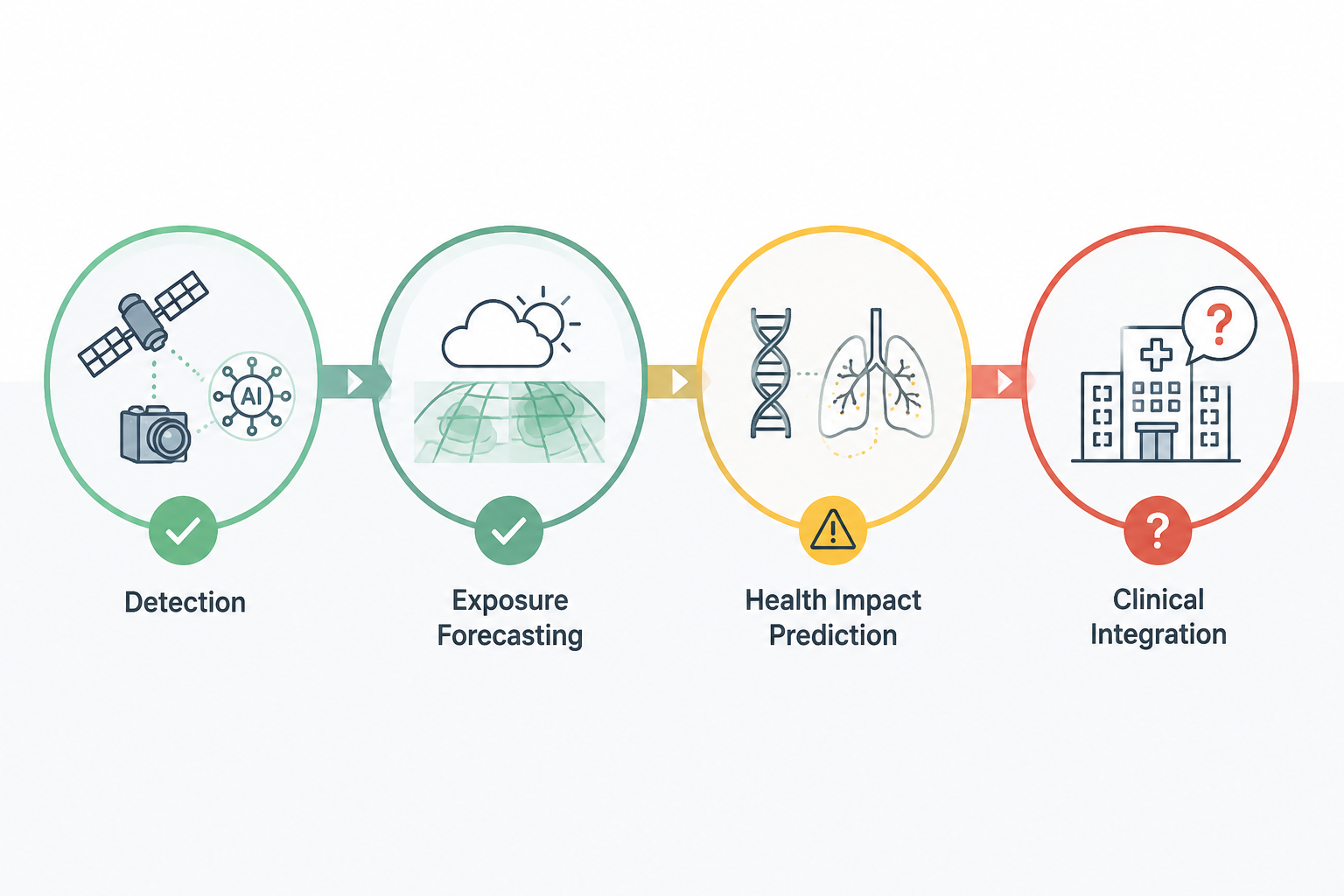
| Pipeline Stage | What AI Is Being Asked To Do | Evidence Posture |
|---|---|---|
| Ignition detection | Identify likely fires quickly from cameras, sensors, or satellite-linked systems | Strongest technical evidence: 95% to 98% detection accuracy, below 2% false alarms, 5 to 10 minutes post-ignition |
| Exposure forecasting | Estimate smoke movement, concentrations, and emissions over hours to weeks | Promising, especially in hybrid ML-chemical transport systems; less certain during rare extreme seasons |
| Pollutant characterization | Move beyond PM2.5 mass toward chemical composition and source-specific hazards | Important for urban smoke and toxicity interpretation, but monitoring coverage is still uneven |
| Health impact prediction | Link exposure mixtures to biological injury or health-risk estimates | Scientifically useful, but not yet sufficient for clinical validation |
| Clinical and public-health integration | Translate alerts into decisions that reduce harm | Weakest evidence link: no demonstrated reduction in emergency visits, hospitalizations, or mortality |
AQI Is Not the Whole Exposure Story
AQI is useful because it is legible. It is also incomplete. A single index can help the public decide whether outdoor air is unhealthy, but it can hide the difference between regional forest smoke and smoke from dense urban combustion. That difference matters for clinicians and public-health officials trying to advise pregnant patients, children with asthma, older adults, outdoor workers, and people with cardiovascular disease.
The urban wildfire concern is not simply “more smoke.” It is a different exposure mixture. Lead, chlorine, benzene, and other combustion products can raise questions that PM2.5 mass alone does not answer.[3] AI monitoring could help here, but only if the data stream includes chemical measurements, source information, or validated inference methods rather than just prettier maps of particle concentration.
For public-health practice, that means a smoke system should be evaluated on the content of the warning. “AQI will be unhealthy tomorrow” may support general protective messaging. “A plume from an urban structure-fire zone is expected to affect these neighborhoods, with concern for toxic combustion products” supports a different conversation about sampling, cleanup, school HVAC decisions, and clinical vigilance.
Health Impact Models Are Useful, but Not Yet Outcome Proof
Health impact prediction is the most tempting part of the pipeline to overstate. It sits close to the question people actually care about: who gets sick, how badly, and whether earlier information changes that trajectory. The evidence is interesting, but it is not the same as showing fewer asthma visits, hospital admissions, cardiovascular events, or deaths.
A 2026 Chem Research in Toxicology study using PySR symbolic regression and DECS scoring identified polycyclic aromatic hydrocarbons, including benzo(k)fluoranthene, as drivers of lung injury, while methoxyphenols such as eugenol and guaiacol appeared as suppressors in the model.[7] The appeal of symbolic regression is transparency: instead of a black-box risk score, it can produce closed-form relationships that researchers can inspect, challenge, and use to generate biological hypotheses.
That transparency is valuable, especially for environmental health science. But the study’s boundaries are substantial. It used female CD-1 mice, with a sample size of 60, exposed through oropharyngeal aspiration of biomass smoke condensate at a single acute time point.[7] That is not chronic human inhalation, not a community smoke episode, and not a clinical decision trial. It can help identify plausible toxic drivers; it cannot prove that an AI monitoring system protects patients.
NOAA has also described AI modeling work on heightened health risks from wildfire pollutants.[8] Such studies can help connect pollutant mixtures with toxicological concern and may improve the risk signals that public-health agencies receive. The same caution applies: modeling heightened risk is not the same evidentiary claim as demonstrating that a warning system reduced downstream illness.
The Missing Link Is the Hand-Off
The weakest part of AI wildfire smoke monitoring is not that the models are useless. It is that the hand-off from model output to health action remains under-validated. A detection alert may go to a fire agency. A plume forecast may go to an air quality dashboard. A health-risk model may sit in a paper or a prototype. Meanwhile, the school nurse, emergency department director, county health officer, dialysis center, outdoor-work supervisor, and asthma clinician need to know what decision is supposed to change.
The integration questions are ordinary and therefore easy to neglect. Who receives the alert after hours? What threshold triggers action? Does the message distinguish uncertainty from urgency? Are hospitals given enough lead time to alter staffing or outreach? Are clinicians told which patients are at elevated risk, or only that the air is bad? Does the public-health agency have authority to act, or only to repost a forecast?
This is where technical validation and public-health validation part ways. A system can detect ignition accurately and still fail to change exposure. It can forecast smoke better than a baseline and still arrive too late for operational decisions. It can identify toxic chemical drivers and still have no pathway into patient care. The missing evidence is not another benchmark alone; it is proof that alerts and forecasts change actions in ways that reduce harm.
What Would Count as Stronger Evidence
For healthcare researchers and health IT teams, the next evidence step is not simply a larger model. It is an evaluation design that follows the warning through real use. A useful study would specify who received the AI alert, what action it triggered, how much lead time was gained, which population was covered, and which clinical or exposure outcome changed afterward.
- For detection systems, the key operational measure is whether earlier ignition recognition leads to earlier smoke advisories, targeted exposure reduction, or faster suppression decisions.
- For exposure forecasts, the key measure is whether agencies act earlier than they would have under existing AQI, weather, or satellite systems.
- For pollutant characterization, the key measure is whether chemical information changes sampling, cleanup, respiratory protection, or clinical guidance.
- For health impact prediction, the key measure is whether risk estimates improve outreach, triage, medication planning, or protection for high-risk groups without widening access gaps.
- For integrated systems, the key measure is whether emergency visits, hospitalizations, mortality, or validated exposure outcomes decline compared with a credible counterfactual.
That last standard is demanding, but it is the standard implied by calling a monitoring system a health intervention. Without it, the more accurate description is narrower: AI is improving parts of wildfire smoke detection, forecasting, and hazard interpretation.
A U.S.-Heavy Evidence Base
The current evidence base represented here is heavily U.S.-centered. That is a limitation, not a minor footnote. Canada, Australia, the Amazon, Southeast Asia, and other wildfire- and smoke-affected regions have different fuels, housing, occupational patterns, public-health authorities, sensor coverage, and clinical access. A model that performs well in one U.S. monitoring environment may not transfer cleanly to another country’s smoke season or health system.
The same applies within the United States. Rural communities, tribal lands, dense urban neighborhoods, agricultural regions, and tourist areas do not experience the same warning options or health-system capacity. AI monitoring can widen or narrow those gaps depending on where sensors are installed, whose data are used to train models, which languages warnings appear in, and whether protective resources exist after the alert.
The Bottom Line for Health Protection
AI wildfire smoke monitoring is no longer just speculative technology. Early fire detection has credible operational numbers: 95% to 98% accuracy, false alarms below 2%, and detection within 5 to 10 minutes after ignition.[4] Exposure forecasting is improving through hybrid modeling and emerging sub-seasonal emissions prediction, though rare extreme seasons remain a hard test.[5][6] Pollutant characterization and health impact modeling are becoming more informative, especially when they move beyond PM2.5 mass alone.[3][7][8]
The health claim has to stop short of the technology claim. No study in this source set demonstrates that AI wildfire smoke monitoring reduces emergency visits, hospitalizations, deaths, or other downstream clinical harms. Until alerts and forecasts are linked to measurable changes in action and outcomes, the pipeline is technically operational and increasingly useful, but clinically unvalidated as a health intervention.
References
- Assessing wildfire health risks, Stanford, 2025.
- Long-term exposure to wildfire smoke associated with higher risk of death, Yale School of Public Health.
- Public health risks of urban wildfire smoke prompt push for more monitoring, News-Medical, 2025.
- Artificial Intelligence: Emerging Opportunities and Challenges for Wildland Fire Management, U.S. Government Accountability Office, 2025.
- AI can help forecast air quality, but freak events like 2023’s summer of wildfire smoke require traditional methods too, The Conversation.
- Artificial intelligence takes wildfire emissions to new frontier of forecasting, CIRES, January 2026.
- Discovery of Chemical Drivers of Biomass Smoke Toxicity through Machine Learning, Chemical Research in Toxicology, 2026.
- Heightened health risks due to wildfire pollutants: Results from an AI modeling study, NOAA Climate Program Office.
Comments
Join the discussion with an anonymous comment.