The patient portal version of this question is usually short: “The AQI is bad today. Can I still run?” In clinic, it may be a parent asking about soccer practice, a patient with coronary disease who walks every morning, a marathon trainee reluctant to miss a long run, or an outdoor worker trying to understand whether a commute by bicycle is foolish. A useful answer cannot be “exercise normally” and cannot be “everyone stay indoors until the smoke is gone.” The first ignores dose and vulnerability. The second often collapses when it meets work schedules, training plans, transportation, housing, and frailty.
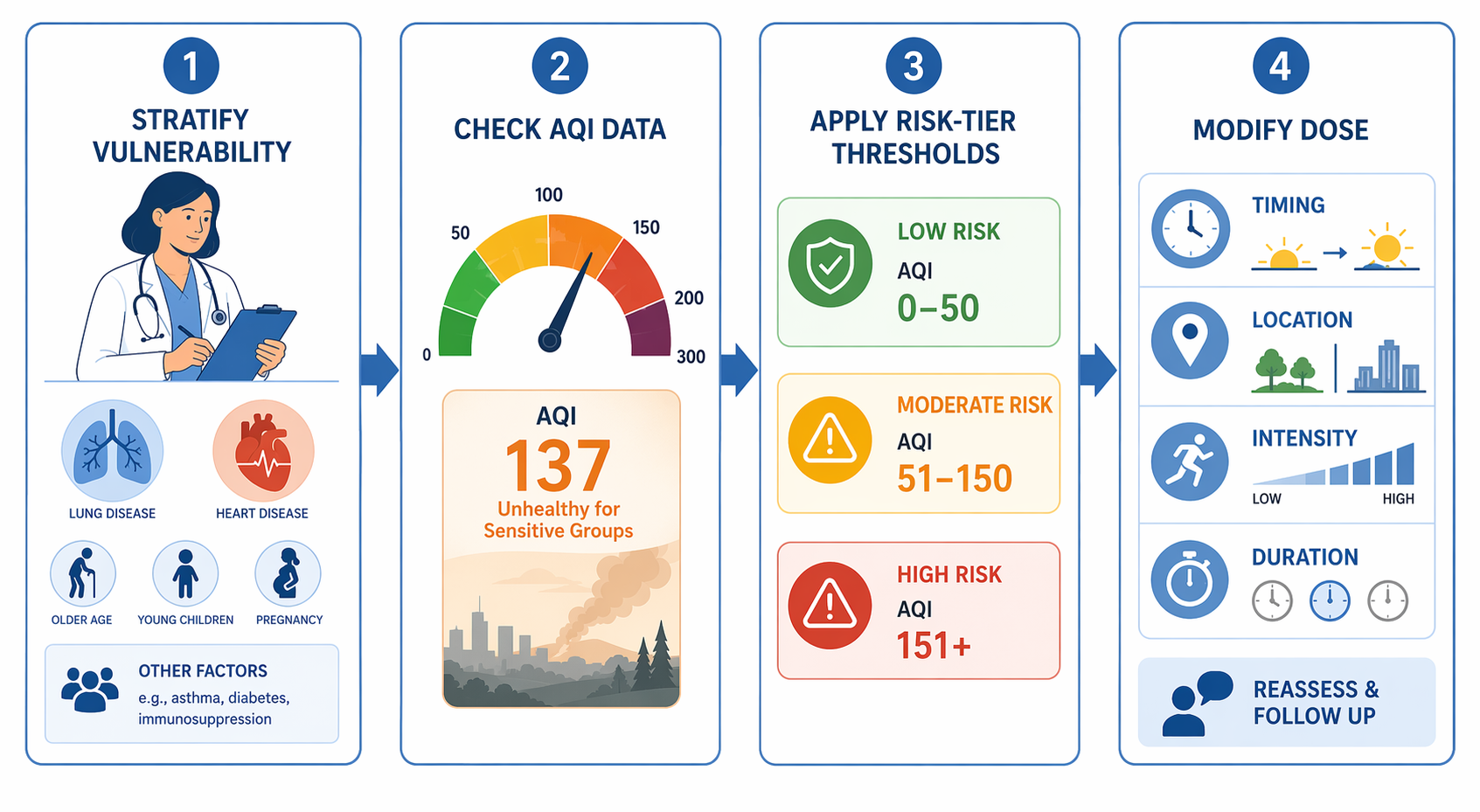
The most clinically useful starting point in Q3 2026 is the 4-step protocol described in CHEST: stratify cardiopulmonary vulnerability, interpret real-time pollutant-specific AQI data, apply AQI thresholds according to risk tier, and then modify timing, location, intensity, or duration rather than treating outdoor activity as a yes-or-no decision.[1] The framework is not a fully validated exercise prescription tool. Its value is more modest and more practical: it gives clinicians a reproducible way to match advice to the patient in front of them.

Why the same smoky day is not the same clinical problem for every patient
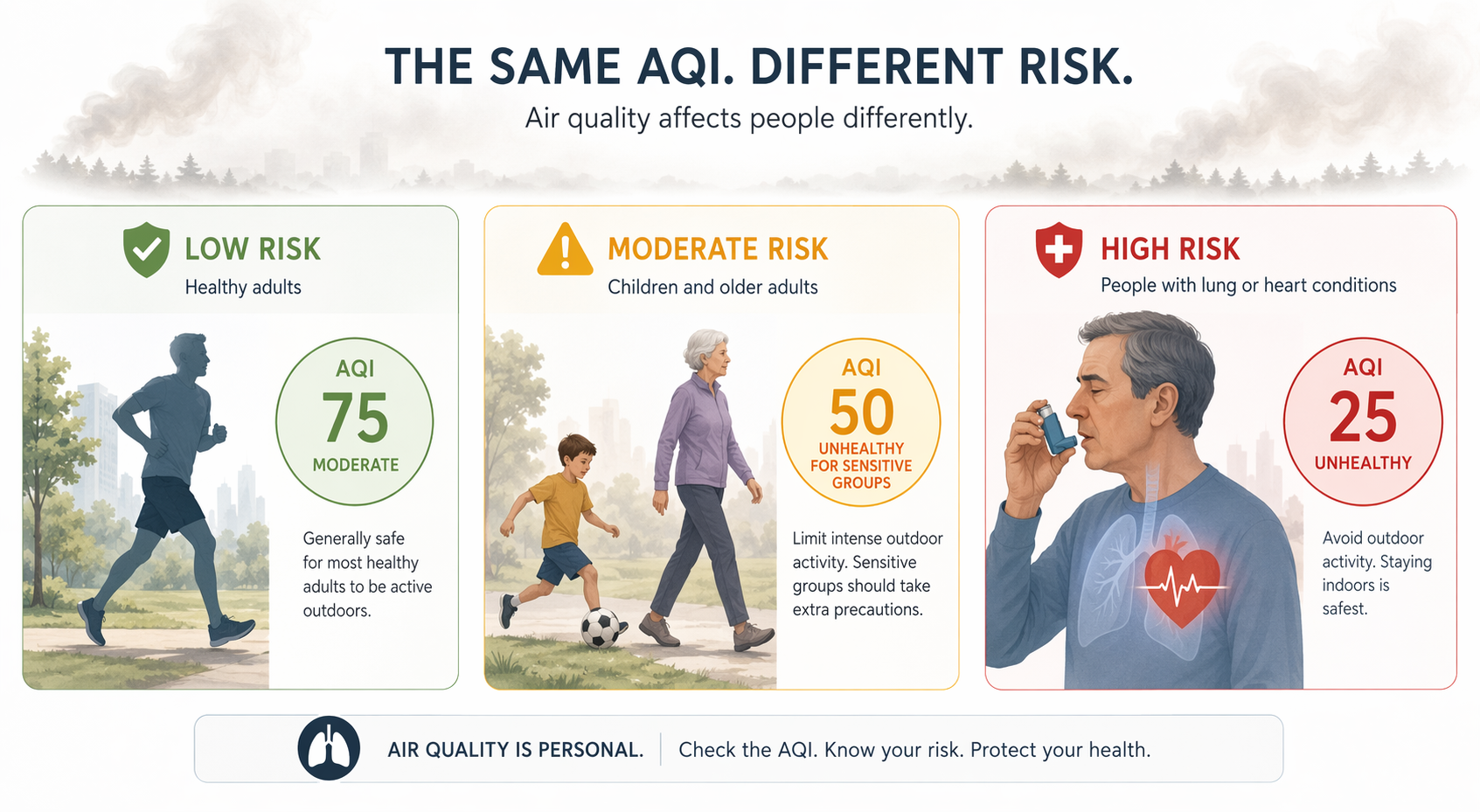
Risk stratification has to come before advice about the run, ride, walk, practice, or shift. The same AQI value does not carry the same meaning for a healthy adult doing a short easy walk, a child at soccer practice, an older adult with heart failure, a pregnant patient, a patient with asthma who has needed oral steroids this year, or someone with known coronary disease. The exposure may be shared; the physiologic reserve is not.
Clinically, “higher risk” should include patients with asthma, COPD, interstitial lung disease, pulmonary hypertension, heart failure, ischemic heart disease, arrhythmia-prone cardiovascular disease, prior stroke, significant pregnancy-related cardiopulmonary concerns, and children or older adults whose symptoms, reserve, or ability to self-monitor are limited. That tier should also include patients whose exposure is hard to control: outdoor workers, people without effective indoor air filtration, patients who rely on walking or cycling for transportation, and athletes whose planned session is unusually long or intense. The last group may look healthy in the chart but can still create a large inhaled dose.
That distinction matters because wildfire-specific PM2.5 is not just ordinary “bad air” with a dramatic sky. A meta-analysis summarized same-day associations between wildfire-specific PM2.5 and acute outcomes: all-cause mortality rose 0.15% per 1 microgram/m3 increase, respiratory hospitalizations rose 0.25%, and respiratory emergency department visits rose 0.36%.[2] Those are population-level associations, not a bedside prediction for one patient. Still, they are enough to make smoke-day exercise counseling a medical issue rather than a lifestyle preference.
There is also evidence that source matters. Stanford reporting in 2025 described wildfire smoke as approximately 10 times more toxic per unit PM2.5 than fossil-fuel combustion sources.[3] That estimate should not be turned into a simple conversion formula for an individual patient, but it is a useful guardrail against underreacting when the AQI number looks merely “moderate” while the local source is wildfire smoke.
Use AQI as a clinical input, not a permission slip
The second step is to check local, current, pollutant-specific air quality data. For smoke events, the clinically relevant value is usually PM2.5, and the patient’s location matters: neighborhood readings, school fields, work sites, commute corridors, and valleys can differ from a regional average. A stale AQI screenshot from early morning is not a reliable guide for an evening workout if winds shift.
AQI should then be interpreted through the patient’s tier. For lower-risk adults planning light or moderate activity, the threshold for changing plans can be higher than it is for a child with asthma or an older adult with coronary disease. For patients with established cardiovascular disease, the American Heart Association recommends avoiding outdoor exercise during polluted conditions; for healthy individuals, it recommends limiting high-intensity exercise when PM2.5 exceeds 55.5 micrograms/m3.[4] That is a useful anchor, but it should not be the only line in the conversation. A patient with unstable angina, poorly controlled asthma, or recent hospitalization deserves stricter advice before the air reaches that level.
| Counseling step | Clinical question | Practical output |
|---|---|---|
| Stratify vulnerability | Who is more likely to be harmed or less able to compensate? | Assign a lower-, intermediate-, or higher-risk counseling tier. |
| Check local data | What is the current PM2.5/AQI where the activity will occur? | Use current, local, pollutant-specific readings rather than regional impressions. |
| Apply tiered thresholds | At this AQI, how strict should advice be for this patient? | Lower the threshold for modifying or avoiding activity as vulnerability rises. |
| Modify dose | Can exposure be reduced without eliminating activity entirely? | Change timing, location, intensity, or duration; cancel or move indoors when risk remains unacceptable. |
Exercise changes the dose
The reason exercise complicates counseling during wildfire smoke is not simply that the patient is outside. Exercise increases minute ventilation. Higher intensity usually means more air moved through the respiratory tract per minute, more oral breathing, and less nasal filtration. Longer sessions add time. A hard 90-minute run in smoke is not equivalent to walking from a parking lot to a clinic entrance, even if both happen under the same AQI reading.
This is where counseling can become more useful than a ban. The modifiable variables are concrete: move the activity earlier or later if the AQI improves, choose an indoor location with better air filtration when available, reduce intensity from intervals to easy effort, shorten the session, split a long workout, substitute strength or mobility work, or postpone the highest-ventilation portion of training. For an outdoor worker or commuter, the equivalent may be reducing exertional load, adding rest periods in cleaner air, changing route or timing, or coordinating workplace accommodations when possible.
A clinician’s wording can stay brief: “Because of your asthma and today’s PM2.5, I would not do hard outdoor exercise. If you need activity, make it short and easy, move it indoors if you can, and use your action plan if symptoms start.” For a lower-risk patient on a borderline day, the advice may be different: “Skip the speed work, shorten the run, and recheck the AQI close to the time you go.” The difference is not indulgence for one patient and alarmism for another. It is dose matching.
What the physiology study can and cannot carry
The controlled exercise evidence is helpful, but it is easy to overuse. In a June 2025 report, 20 healthy adults in their mid-20s exercised for 2 hours in simulated wildfire smoke and showed acute declines in vascular and autonomic function. Those effects resolved within 1 hour in clean air, while stress-responsive individuals had significantly stronger effects.[5] That finding supports biological plausibility: smoke exposure during exercise can affect cardiovascular regulation even in young healthy adults.
It does not prove that every adult should stop all outdoor activity during every smoke event. It also does not reassure us about patients who are older, pregnant, children, have asthma, have COPD, have cardiovascular disease, or cannot recover in clean air after exposure. The sample was small, the participants were healthy, and the recovery window was short.[5] Clinically, the study belongs in the middle of the argument: strong enough to discourage casual reassurance, not strong enough to replace risk-tiered judgment.
A two-minute counseling script that preserves proportion
In practice, the framework can fit into a short visit or message if the clinician resists explaining every branch of the evidence. The patient needs to know their tier, the current pollutant concern, the action threshold, and the modification plan. The chart should capture enough detail that another clinician would give similar advice the next day.
- Name the vulnerability: “Your heart disease puts you in a stricter group for smoke-day exercise.”
- Name the pollutant: “Today’s concern is PM2.5 from wildfire smoke, not just heat or pollen.”
- Name the dose change: “No hard intervals outside today; if you exercise, keep it short and easy or move indoors.”
- Name the escalation point: “If you develop chest pain, unusual shortness of breath, wheeze not responding to your plan, dizziness, or palpitations, stop and seek care according to your usual emergency instructions.”
The phrase “listen to your body” is not enough. Some patients do notice wheeze, chest tightness, cough, or unusual fatigue quickly. Others may not feel the cardiovascular or autonomic effects that matter during exposure. Symptom awareness is useful as a safety net, not as the primary exposure-control strategy.
When the honest answer is that outdoor exercise should wait
Risk-stratified counseling is not a way to keep everyone outside. Some combinations should lead to postponement or indoor substitution: high PM2.5 with a patient who has unstable cardiopulmonary disease, recent exacerbation, poor symptom control, high-intensity planned exercise, prolonged duration, or no realistic recovery environment. The same applies when the patient’s role makes self-monitoring unreliable, such as a child in a competitive setting where they may not stop when symptoms begin.
Institutions should be especially careful here. A public advisory that says “stay indoors” may be medically appropriate on severe days, but it is incomplete if it leaves patients and workers to solve the implementation problem alone. A sports program needs cancellation and relocation rules. A clinic needs message templates. An employer needs a plan for outdoor work. A frail patient needs a safe alternative to the daily walk if that walk is part of fall prevention, mood management, or glucose control.
The evidence gap clinicians should not hide
There are no randomized controlled trials that settle exercise-specific outcomes during wildfire smoke events. The current counseling base is built from observational epidemiology, cardiovascular and respiratory air pollution evidence, and small controlled exposure studies. The CHEST protocol is clinically useful, but the available description is abstract-level rather than a fully accessible, externally validated decision rule.[1] That matters when turning it into institutional policy.
The other unresolved problem is scale. Acute high-AQI days demand immediate counseling because the risk is visible and decisions are time-sensitive. Yet chronic low-to-moderate exposure may create a larger total population burden than the most dramatic smoke days, precisely because more people experience it more often. Clinical guidance tends to focus on the red-flag day; public health planning has to account for the many days that never trigger a crisis message.
For now, structured AQI-based risk stratification is the best available clinical approach: identify vulnerability, verify local PM2.5 conditions, lower thresholds as baseline risk rises, and prescribe specific changes to timing, location, intensity, and duration. It is not complete evidence. It is a more honest and usable answer than pretending smoke does not matter or treating every patient’s outdoor life as disposable.
References
- CHEST 2026 clinical protocol on wildfire smoke and exercise, ScienceDirect, 2026, link
- Wildfire Smoke Exposure and Human Health: Significant Gaps in Research for a Growing Public Health Issue, Annual Review of Medicine, 2024, link
- Assessing wildfire health risks, Stanford Report, 2025, link
- Personal-Level Protective Actions Against Particulate Matter Air Pollution Exposure: A Scientific Statement From the American Heart Association, Circulation, 2022, link
- Wildfire smoke can make your outdoor workout hazardous to your health — an exercise scientist explains how to gauge the risk, The Conversation, June 2025, link
Comments
Join the discussion with an anonymous comment.