The State of Clinical AI 2026 report stopped me cold: more than 1,200 FDA-cleared devices, a multibillion-dollar industry, studies where AI beats physicians on standardized tests. But of the 500+ studies surveyed, nearly half tested models on exam-style questions. Only five percent used real patient data. That five percent is the gap between what the headlines claim and what the evidence actually supports.
Catching deterioration hours before anyone else
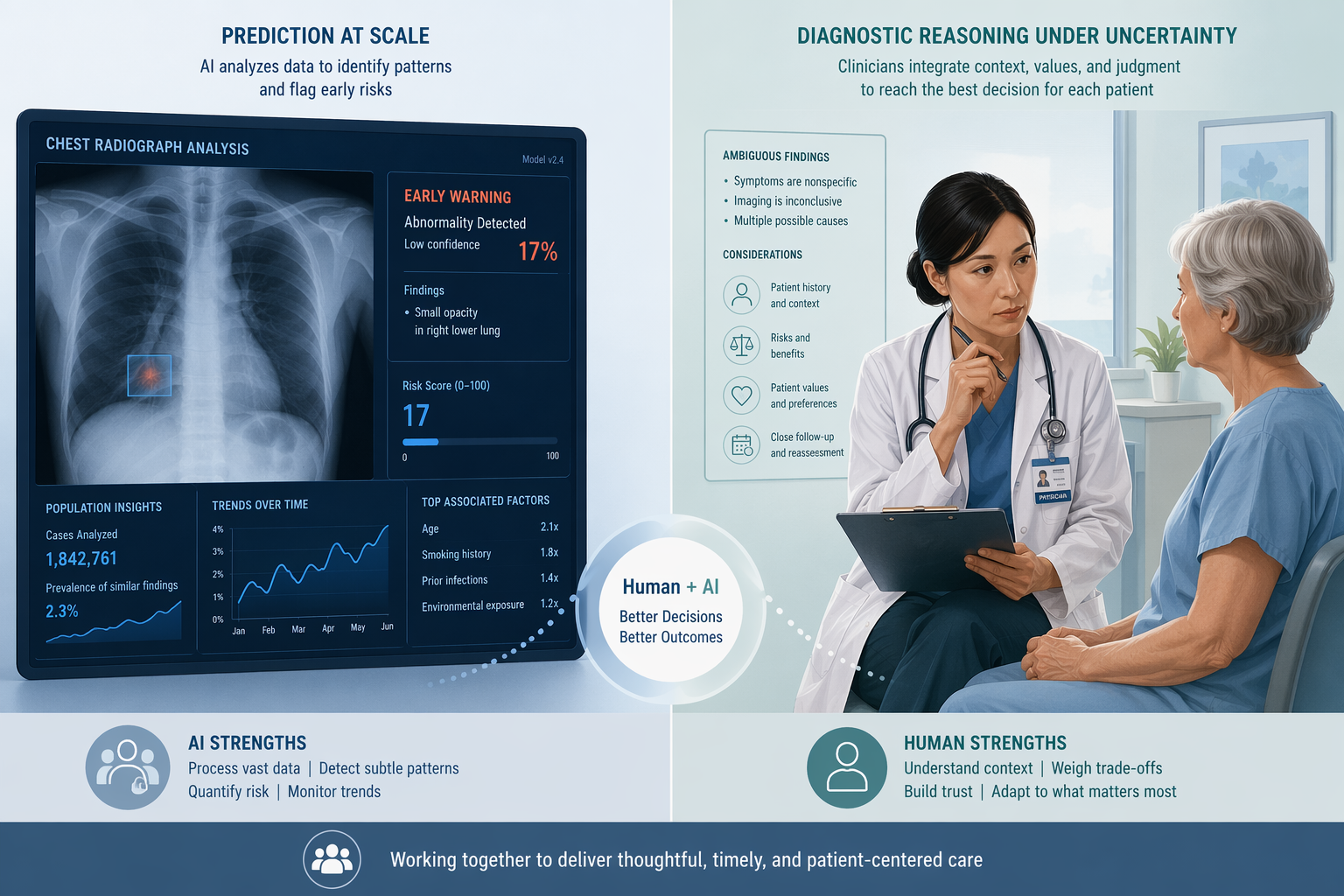
Start with what works. A model trained on continuous wearable vital signs predicted patient deterioration 8 to 24 hours before standard hospital alerts triggered — earlier warnings for ICU transfer, cardiac arrest, or death. That is a task where AI has an inherent advantage: it processes high-frequency, multi-dimensional data without fatigue, and it acts on clear clinical signals like heart rate variability and oxygen saturation trends that no human can track continuously. The study in Nature Communications tested the model on real ward data from multiple hospitals. Not a lab exercise.
Another example: researchers estimated “biological age” from routine health records across millions of individuals. The AI-derived age measure predicted mortality more accurately than epigenetic clocks and frailty scores. Again, prediction at scale — not reasoning about a single patient, but identifying population-level patterns that no human analyst could feasibly discover.
These are not small effect sizes. The deterioration model extended the warning window by nearly a full day — enough time to intervene and reduce mortality. If I were a health system leader, I would invest in this kind of predictive AI today.
Then the none-of-the-above problem broke every model
Then came the experiment that should give every optimist pause. Researchers took standard medical multiple-choice questions and modified them so the correct answer became “none of the other answers.” Accuracy dropped sharply across leading AI systems — in some cases by more than a third. This was not a trick. It mimics a situation every clinician faces: when the correct diagnosis is not in the differential you were given, or when the patient's presentation doesn't fit a textbook category.
I don't buy the argument that multiple-choice tests are irrelevant. They are revealing. They show these models have learned to match patterns in the training data, but they have not learned the underlying structure of clinical reasoning. Remove the pattern they expect, and they fail.
A meta-analysis of 83 studies published in npj Digital Medicine puts generative AI’s pooled diagnostic accuracy at 52.1%. But 76% of those studies were rated high risk of bias. I wouldn't take the 52.1% as precise — the underlying quality is too uneven. But the pattern is consistent: when evaluation reflects real clinical conditions — uncertain presentations, evolving information, multiple plausible explanations — AI’s advantage vanishes.
The FDA device landscape reinforces the same point. Out of 736 unique AI devices authorized through September 2024, 84.4% rely on images. No large language models had been authorized as medical devices at that point. The field is dominated by pattern recognition in imaging, not diagnostic reasoning. And among those cleared devices, 43% of recalls happened within one year of authorization. The validation gap is not theoretical.
When AI works as a teammate, not a replacement
None of this means AI is useless in diagnosis. It means the deployment model matters. A study in Germany gave radiologists the option to consult an AI system during mammography reading. Those who used it detected more cancers without increasing false alarms. The key word is optional. The radiologist could overrule the AI, ignore it, or use it as a second look. That preserved human judgment for ambiguous cases.
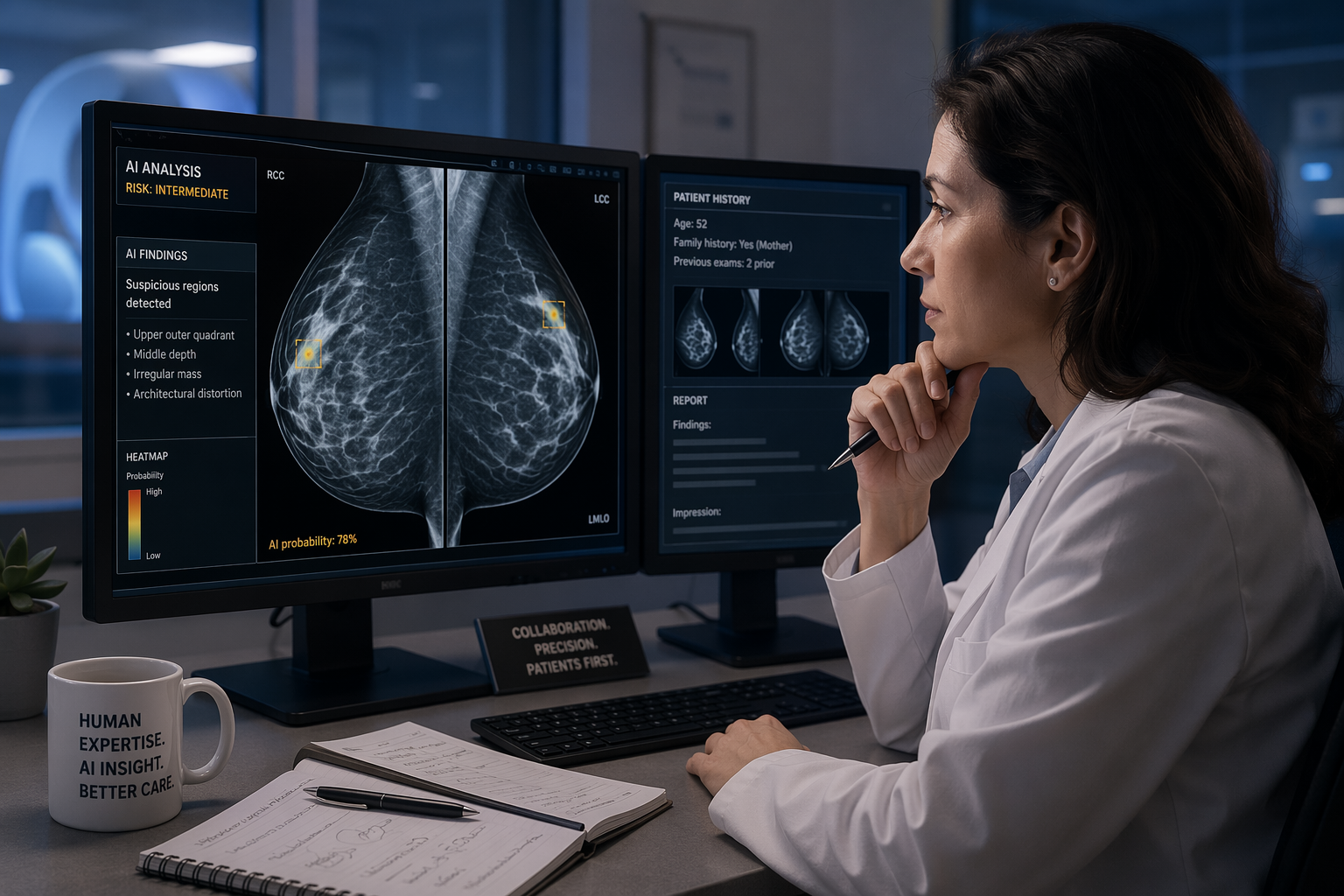
This contrasts with the AI‑alone paradox: when physicians are forced to rely on AI, they often underperform the AI working independently. The difference is autonomy. The human can choose when to trust the machine; when the machine's output is treated as authoritative, errors propagate.
The o1 model's early emergency department performance — identifying the correct diagnosis 67% of the time versus 50–55% for physicians — sounds dramatic. But the study used curated, well-documented cases. That is not the same as a real ED shift where patients come in without a clear history and the differential evolves over hours. Even o1's reported 98% reasoning score on those curated cases should be interpreted cautiously: it tells us what the model can do under ideal conditions, not what it does when the data is messy.
Invest in prediction, be cautious with reasoning
Health systems face a practical choice. The evidence supports deploying AI for prediction-at-scale tasks — early deterioration warnings, risk stratification, screening prioritization. These tools have real-world validation, clear workflows, and measurable impact. The same evidence does not support deploying AI as an autonomous diagnostic reasoner in settings with incomplete or evolving information.
- Invest now in predictive AI that flags deterioration, estimates biological age, or prioritizes imaging reads. The evidence for clinical benefit is solid when the tool is designed as a support system, not a decision maker.
- Avoid deploying current LLM‑based tools for diagnostic reasoning in ambiguous cases — patients with multiple potential diagnoses, incomplete records, or evolving presentations. The evaluation methods do not yet reflect those conditions.
- Build workflows that keep the human in the loop with the authority to override. The teammate effect works because the physician can ignore the AI when they suspect it is wrong.
- Treat every FDA clearance as a starting point, not a guarantee. With 43% of recalls within one year, post‑market surveillance is not optional.
I have seen enough inflated claims to know that the prediction-vs-reasoning distinction is not a nuance. It is the difference between a tool that helps and one that harms. The State of Clinical AI 2026 report draws that line clearly. The rest is up to the people who decide what gets deployed and how.
Comments
Join the discussion with an anonymous comment.