The No-Show Crisis by the Numbers
Missed appointments are not a minor operational nuisance — they represent a structural drain on clinical capacity and practice revenue that has resisted conventional solutions for decades. Across US outpatient settings, baseline no-show rates range from 15% to 30%, depending on specialty, patient population, and geographic factors. The aggregate cost to the healthcare system is estimated at $150 billion annually, a figure that accounts for lost clinical time, idle staff, and the downstream effects of delayed care.
The financial impact varies sharply by specialty, driven by differences in reimbursement rates, procedure complexity, and patient demographics. A 2025 study published in the Journal of General Internal Medicine (cited in the Neuwark analysis) provides a per-specialty breakdown that helps administrators prioritize where AI-based interventions deliver the highest return.
| Specialty | No-Show Rate Range | Cost per No-Show | Annual Loss (Solo Practice) |
|---|---|---|---|
| Primary Care | 18–23% | $205 | $120K–$155K |
| Behavioral Health | 25–30% | $190 | $140K–$175K |
| Pediatrics | 20–28% | $195 | $115K–$160K |
| Dermatology | 15–20% | $275 | $110K–$145K |
| OB/GYN | 16–22% | $310 | $135K–$185K |
| Orthopedics | 12–18% | $385 | $130K–$190K |
| Dental | 15–25% | $250 | $100K–$170K |
Behavioral health and pediatrics carry the highest no-show rates — exceeding 25% in many practices — while orthopedics and OB/GYN incur the steepest per-appointment losses due to higher reimbursement for procedures and consultations. For a multi-provider practice, these losses compound quickly. A five-provider primary care clinic with a 22% no-show rate and an average revenue of $250 per appointment is looking at roughly $36,250 in lost revenue per month, or $435,000 annually, before any intervention costs.
Why Traditional Reminders Fall Short
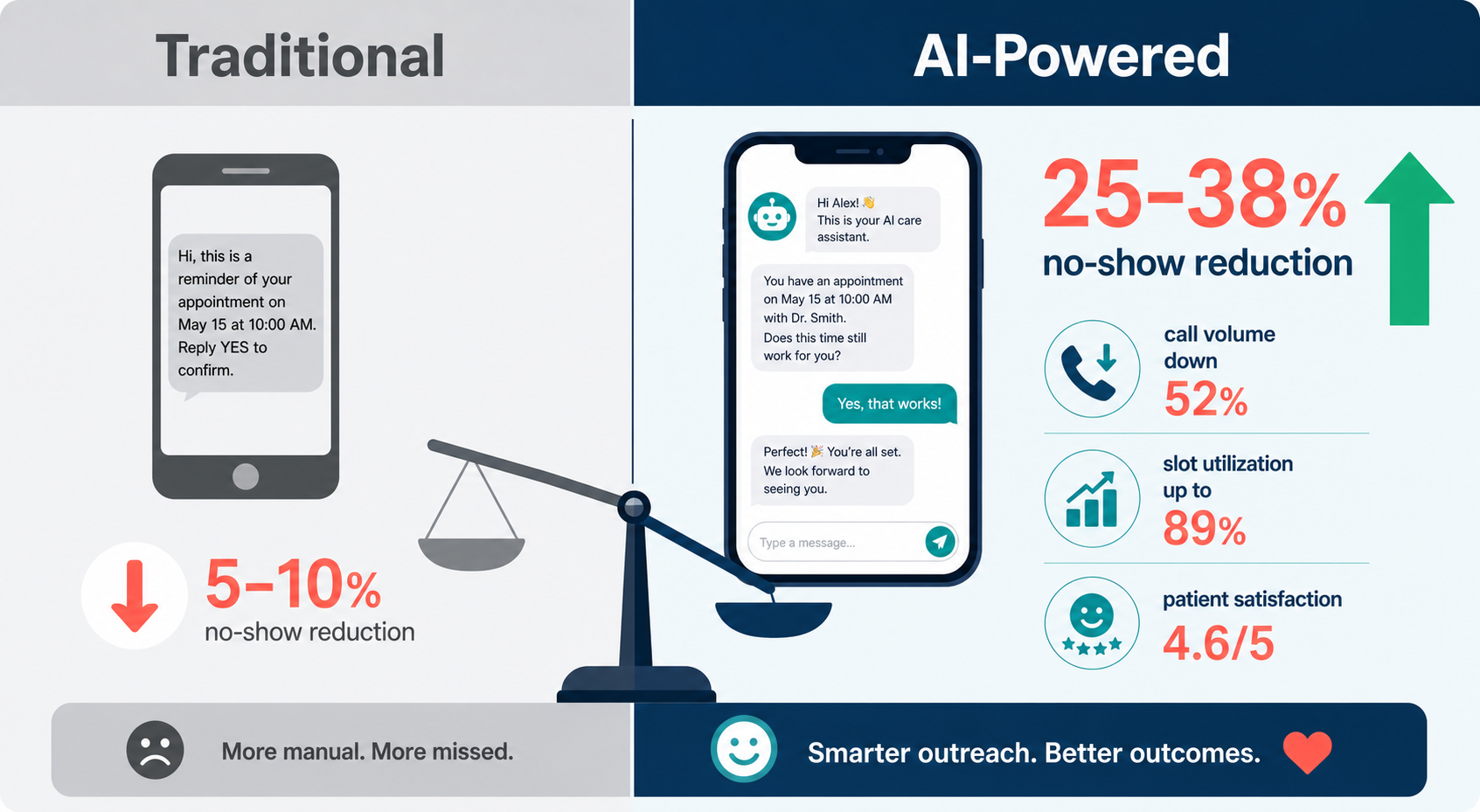
Most practices already use some form of appointment reminder — automated SMS, email, or phone calls. These systems are inexpensive and easy to deploy, but their impact on no-show rates is modest at best. Published data consistently shows that standard reminders reduce missed appointments by only 5% to 10%, leaving the vast majority of the problem untouched.
The limitations are structural, not technological. Traditional reminders are one-directional: they deliver a fixed message at a fixed time and cannot respond to patient questions, accommodate rescheduling requests, or handle the complex logistics that drive no-shows in the first place. Consider the following gaps:
- 68% of appointment-related patient inquiries occur outside business hours (Neuwark, citing industry data). A reminder sent during the day is useless if the patient has a question at 9 PM.
- SMS and email cannot handle multi-turn conversations. If a patient needs to reschedule, confirm insurance coverage, or ask about pre-visit instructions, they must call the office — which is often closed or understaffed.
- No personalization. Standard reminders treat every patient the same, ignoring differences in preferred communication channel, language, or the specific barriers that cause that patient to miss appointments.
- No progressive engagement. A single reminder sent 24 hours before an appointment cannot adapt if the patient has a history of no-shows or if the appointment is high-value (e.g., a procedure requiring preparation).
These gaps are not hypothetical. The 5–10% reduction ceiling means that a practice with a 25% no-show rate is still losing 15–20% of appointments after implementing standard reminders. The remaining gap represents patients who need more than a notification — they need a conversation.

How Conversational AI Works in Practice
Conversational AI platforms for patient engagement differ from standard reminder systems in three fundamental ways: they are interactive, adaptive, and available continuously. Rather than sending a static message, these systems use natural language processing (NLP) to engage patients in a dialogue that can handle scheduling, pre-visit intake, insurance questions, and clinical triage — all without human intervention for routine cases.
The typical workflow operates across multiple touchpoints:
- Initial outreach: The AI sends a personalized message via the patient's preferred channel (SMS, email, or app notification) confirming the appointment and inviting questions.
- Progressive intake: If the patient responds, the AI collects pre-visit information — medication lists, symptom updates, insurance changes — reducing the administrative burden on front-desk staff and clinicians.
- Rescheduling and cancellation: Patients can reschedule or cancel directly through the conversational interface. Critically, the AI can offer alternative slots in real time, keeping the appointment in the schedule rather than losing it entirely.
- After-hours resolution: Because the system operates 24/7, patients who have questions at night or on weekends can get immediate answers rather than waiting until the next business day.
- Human escalation: When the AI encounters a question it cannot handle — a clinical concern, a complex billing issue, or a patient request for a human — it routes the interaction to the appropriate staff member with full context preserved.
The multi-touch approach is what drives the step-change in no-show reduction. A single reminder is easy to ignore. A conversational system that follows up, asks clarifying questions, and makes it easy to reschedule rather than simply cancel creates a fundamentally different patient experience. Data from Revenue Care AI's CareFlow AI platform, reported in the Neuwark analysis, shows that 88% of patients who used AI rescheduling kept their rescheduled appointment, compared to 62% for phone-rescheduled appointments.
Clinical Outcome Data from 2025–2026 Implementations
The most detailed before-and-after data available comes from deployments of Revenue Care AI's CareFlow AI platform, as reported in a March 2026 analysis by Neuwark. The table below summarizes the pre- and post-implementation metrics across a range of operational and clinical dimensions.
| Metric | Before AI | After AI | Change |
|---|---|---|---|
| Overall no-show rate | 23.4% | 14.8% | −37% |
| Same-day cancellation rate | 11.2% | 7.1% | −37% |
| Pre-visit intake completion | 22% | 78% | +255% |
| Average check-in wait time | 18 min | 4 min | −78% |
| After-hours inquiry resolution | 0% | 94% | N/A |
| Patient satisfaction (scheduling) | 3.2 / 5 | 4.6 / 5 | +44% |
| Staff phone call volume | Baseline | −52% | −52% |
| Appointment slot utilization | 71% | 89% | +25% |
Several findings merit close attention. The 37% reduction in no-shows is consistent with the 25–38% range reported across multiple implementations, and the 52% drop in call volume suggests that the AI is handling a substantial portion of routine inquiries that would otherwise tie up front-desk staff. The improvement in intake completion — from 22% to 78% — is particularly notable because incomplete pre-visit information is a known driver of workflow inefficiency and clinician burnout.
Beyond no-show reduction, the PwC case study of a national nonprofit health system deploying an AI-powered contact center across 50+ sites reported an 85% decrease in call abandonment rate and over 3,000 hours saved per month. While that deployment focused on broader patient engagement — including nurse triage and patient verification — the call-volume reduction directly supports the case that conversational AI can meaningfully offload administrative burden from clinical staff.
ROI Framework for Solo and Multi-Provider Practices
The financial case for conversational AI in no-show reduction rests on a straightforward calculation: the revenue recovered from filled appointment slots minus the cost of the AI platform. The Neuwark analysis provides a concrete model for a five-provider practice.
| Parameter | Value |
|---|---|
| Number of providers | 5 |
| Baseline no-show rate | 22% |
| Average revenue per appointment | $250 |
| Monthly appointments per provider | ~220 |
| Monthly lost revenue (baseline) | $36,250 |
| No-show reduction with AI (30%) | ~$10,875/month recovered |
| Annual recovered revenue | ~$435,000 |
| Typical AI platform cost (monthly) | $1,500 – $3,000 |
| Estimated payback period | < 30 days |
The payback period of under 30 days is driven by the low fixed cost of AI platforms relative to the revenue recovered. Even a solo practitioner with a 22% no-show rate and $205 per appointment (the primary care average) stands to recover roughly $10,000–$12,000 annually after platform costs — a meaningful return for a single-provider practice operating on thin margins.
It is important to note that the ROI calculation above captures only direct revenue recovery from reduced no-shows. It does not include secondary benefits such as reduced staff overtime from lower call volume, improved patient satisfaction scores (which correlate with retention and referrals), or the operational value of higher slot utilization. When these factors are included, the total return is likely higher than the direct revenue model suggests.

Implementation Considerations
Deploying conversational AI for patient engagement is not a plug-and-play operation. Several factors determine whether a practice achieves the outcomes described above or struggles with low adoption and integration failures.
HIPAA Compliance and Data Security
Any AI platform handling patient scheduling, intake, or clinical communication must be HIPAA-compliant. This means the vendor must sign a Business Associate Agreement (BAA), encrypt data in transit and at rest, and provide audit logs for all patient interactions. Practices should verify compliance documentation before deployment, not assume it.
EHR Integration Requirements
The AI system must integrate with the practice's electronic health record (EHR) to access appointment schedules, patient contact information, and clinical data for intake. Integration complexity varies by EHR vendor and platform. Practices using major systems like Epic, Oracle Health (Cerner), or Athenahealth typically have more integration options, while smaller or custom EHRs may require additional development work. The PwC case study deployment, for example, used Salesforce Health Cloud as the integration layer, which may not be available or cost-effective for smaller practices.
Specialty-Specific Configuration
No-show patterns and patient communication needs differ by specialty. A behavioral health practice with a 30% no-show rate and patients who may need extra encouragement to attend appointments requires a different engagement strategy than an orthopedics practice where patients are highly motivated but may need detailed pre-procedure instructions. The AI platform should allow customization of message timing, tone, escalation rules, and intake questions by specialty or even by individual provider.
Human Escalation Pathways
No AI system can handle every patient interaction. The Cureus study covered by Healthcare IT News emphasizes that effective systems employ clinicians to review all content and interactions, with triggers for human-in-the-loop escalation. Patients must be able to request a human clinician at any time. The escalation pathway should be clearly defined before deployment: which staff members handle which types of escalations, what the response time target is, and how the AI transfers context to the human without requiring the patient to repeat information.
Staff Training and Change Management
Front-desk staff and clinical teams need training on how to work alongside the AI system. The 52% reduction in call volume means fewer routine inquiries, but the calls that do come through are likely to be more complex — requiring staff to handle higher-level issues rather than simple scheduling questions. This shift can be unsettling for staff who are accustomed to a certain workflow. Clear communication about how the AI changes roles, rather than eliminating them, is essential for adoption.
Limitations and Caveats
The evidence for conversational AI in no-show reduction is promising, but it is not without important limitations that practices should weigh before making procurement decisions.
Digital Divide and Older Patient Adoption
Conversational AI systems rely on patients having access to a smartphone, internet connectivity, and the digital literacy to interact with a chatbot. Older adults, patients in rural areas with limited broadband access, and those with lower health literacy may struggle to use these systems effectively. The 88% patient satisfaction score reported for AI scheduling may not generalize to populations with lower digital engagement. Practices serving a high proportion of older or underserved patients should plan for alternative communication channels and ensure that the AI system can fall back to phone-based or in-person support.
Data Quality and Verification Gaps
As noted throughout this article, the most detailed outcome data comes from vendor-collected sources rather than independent peer-reviewed studies. The Neuwark analysis is a vendor blog. The PwC case study, while more independent, is still a consulting firm's account of its own client work. The Cureus study on chatbot engagement for chronic disease — which reports that AI systems achieve engagement rates over 90% and care plan adherence as high as 97% — is peer-reviewed but was accessed through secondary coverage (Healthcare IT News) rather than direct reading due to paywall restrictions. Independent, multi-center randomized controlled trials are needed to confirm these results across diverse practice settings and patient populations.
The Cureus study context is worth noting separately. Dr. James Colbert, CMO at Commure (Memora Health), stated in the Healthcare IT News coverage that on average only half of patients with chronic disease adhere to care plans and medications. Memora Health's conversational AI system achieves engagement rates over 90% for enrolled patients, with some clients seeing care plan adherence rates as high as 97%. While these figures are impressive, they apply to a different use case — chronic disease management — rather than appointment attendance. The overlap is that both use cases rely on sustained patient engagement, but the mechanisms and patient populations differ.
Market Sizing Context
The broader AI in patient engagement market is projected to grow from $11.28 billion in 2026 to $24.74 billion by 2030, at a compound annual growth rate (CAGR) of 21.7%, according to ResearchAndMarkets. North America was the largest region in 2025, and Asia-Pacific is expected to be the fastest-growing region. These figures provide useful context for the scale of investment and adoption, but they are market research estimates based on aggregated secondary sources, not primary data. They should not be cited as evidence of clinical efficacy.
Despite these caveats, the convergence of evidence across multiple sources — vendor data, consulting case studies, and peer-reviewed research — suggests that conversational AI is a genuinely effective tool for reducing no-shows in outpatient settings. The 25–38% reduction range is consistent across implementations, the ROI payback period is unusually short for healthcare technology investments, and the secondary benefits (reduced call volume, improved intake completion, higher patient satisfaction) address multiple pain points simultaneously. For practices that can navigate the implementation requirements and account for the digital divide, conversational AI represents one of the most immediately actionable applications of AI in clinical operations today.
Comments
Join the discussion with an anonymous comment.