What Problem Are You Solving?
The best question to ask about AI in primary care is not “which tool should I adopt?” It is “what problem am I trying to solve?” Stanford Medicine’s HEA₃RT framework makes this distinction explicit: start with the clinical need. In primary care, five pain points are so well-documented that they almost define the specialty’s current crisis. Chart review consumes 33% of EHR time. Medical knowledge doubles every 73 days. Patients remember only 49% of what they are told. Documentation overload drives burnout. Portal messages have surged 1.6-fold since the pandemic. Each of these has a matching AI solution — but the evidence for those solutions is uneven. I want to walk through each one, say what the number actually measures, and where I think the claims outrun the data.
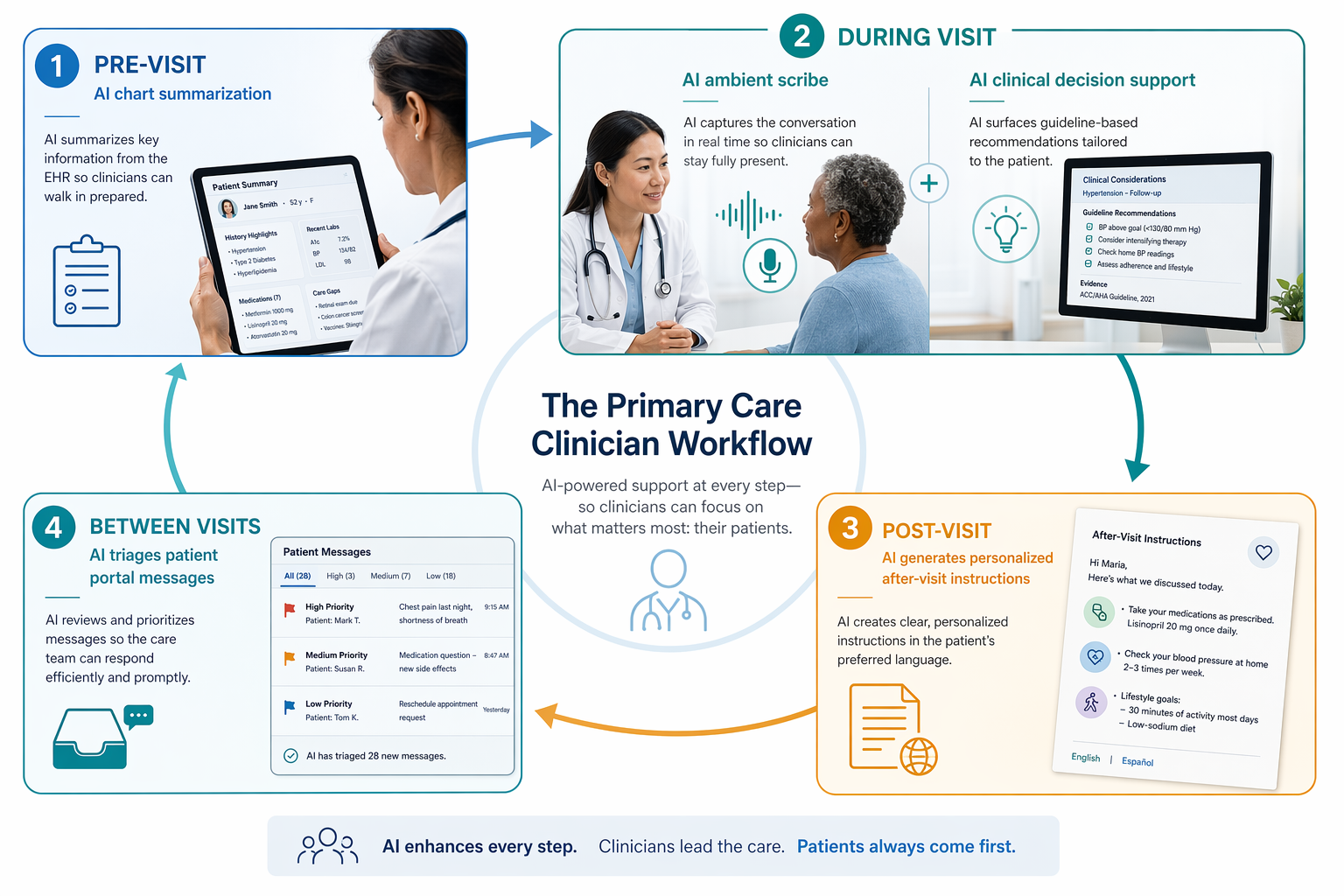
Chart Review: The 33% You Cannot Recover Entirely
A 2024 study in the Journal of General Internal Medicine found that chart review accounts for 33% of ambulatory physicians’ EHR time. That number comes from a time-motion study — not a survey. It is solid. But I would not treat it as a promise that AI summarization can recover the entire 33%. The study measured all EHR time: scrolling, reading, thinking, cross-referencing. AI can speed the reading part — a 2021 JAMA study showed that AI can accelerate chart review without sacrificing accuracy — but the thinking and cross-referencing remain. Even so, shaving even part of that 33% would be meaningful. The question is whether current tools deliver that in real clinics, not just controlled studies. As our own analysis of the evidence gap in primary care AI notes, technical performance has not yet translated to measurable clinical impact in many domains. Chart summarization may be the exception, but the evidence is still early.
Clinical Decision Support: The 73-Day Doubling Figure Is an Illustration, Not a Fact
I have seen the projection that medical knowledge doubles every 73 days cited as a hard fact. The original source was an opinion piece. Treat it as a compelling illustration. The underlying problem is real: it takes an average of 17 years for new evidence to change practice, and fewer than 25% of heart failure patients were on guideline-directed therapy by 2020. AI-powered clinical decision support tools promise to surface relevant recommendations at the point of care. The evidence for these tools in primary care, however, is thinner than promotional materials suggest. Most published studies are before-after designs or funded by tool vendors. The evidence gap article on this site covers the details. For now, the prudent stance is: CDS is promising but should be adopted with a monitoring plan that measures whether it actually changes prescribing or referral decisions.
After-Visit Instructions: Accuracy Is Not Recall
Patients remember only 49% of what they are told during a visit. AI-generated after-visit instructions, personalized to the patient’s language and context, seem like an obvious fix. A 2022 NeurIPS study found that physicians rated AI-drafted instructions as more accurate and helpful than standard handouts. But note what was measured: physician rating, not patient recall or adherence. A draft can be clinically perfect and still not improve what the patient remembers. I do not mean to dismiss the approach — personalized instructions are a clear improvement over generic sheets — but the evidence for actual patient outcomes is not yet there. The NeurIPS study is a solid proof of concept; the next step is to test on comprehension and adherence.
Ambient AI Scribes: The Time-Savings Claims Are All Over the Map
Documentation burden is the pain point everyone feels. Ambient AI scribes listen to the encounter and generate a note. The evidence on time savings is famously mixed. The most robust independent data comes from The Permanente Medical Group: 84% of physicians reported a positive effect on communication, 56% of patients noted an improved visit, but the actual time saved was only 18 seconds per appointment. Mass General Brigham saw a median reduction of 5.6 minutes per appointment. A vendor survey funded by Suki (reported by Fierce Healthcare) claimed 60% burnout reduction and 41% notetaking time reduction among 116 small-practice physicians. The contrast is instructive. The common thread across the independent studies is not large time savings but improved visit quality and reduced cognitive load. I would be careful about purchasing a scribe based on vendor time-savings claims; ask instead how it affects the patients’ and clinicians’ experience of the visit.
Portal Message Triage: Less Mental Load, Same Inbox Size
The post-pandemic surge in patient portal messages — a 1.6-fold increase — has added a new layer of async work to primary care. AI draft reply systems aim to reduce that burden. A 2024 study in JAMA Network Open found that within five weeks, clinicians adopted AI-generated draft replies for about 20% of messages. Burnout measures improved, but there was no reduction in time spent. This is a nuanced result: automation does not yet shrink the inbox, but it shifts the cognitive burden from composing replies to reviewing and editing drafts. The 20% adoption rate, while modest, suggests that clinicians find drafts useful for certain types of messages. For a deeper look at safety and governance considerations, see our article on generative AI for patient portal messaging. In brief: portal message triage is a promising area, but the evidence shows it is a tool for reducing mental effort, not for clearing inboxes faster.
Where to Start
Having mapped five pain points to five AI solutions, the question becomes: where to start? The framework suggests a straightforward path.
For a more systematic approach, see our framework for evaluating AI tools in clinical practice. And for a deeper look at why so many promising pilots fail to scale, read about barriers and success factors for deploying conversational AI in clinical workflows. The goal is not to adopt AI for its own sake. It is to solve a specific, documented problem — and then measure whether the solution actually changed the thing that mattered.
Comments
Join the discussion with an anonymous comment.