CDC gastrointestinal outbreak investigation protocols are not built around a single moment of discovery. They are built around a sequence of judgments: noticing an unusual signal, deciding who counts as a case, asking what exposures connect those people, testing whether the pattern holds, confirming the source, stopping ongoing transmission, and deciding when the event has ended. CDC describes acute enteric outbreak investigation as a dynamic process, and its public investigation steps page lays out the familiar seven-part flow: detect, define cases, generate hypotheses, test hypotheses, confirm the source, stop the outbreak, and determine when it is over.[1][2]
AI fits into that workflow only when it helps one of those judgments happen earlier, with better linkage, or with a clearer next action. A model that flags emergency department symptoms, clusters whole genome sequencing results, classifies a probable pathogen, or forecasts a norovirus trajectory is not “finding the outbreak” by itself. It is changing the queue in front of epidemiologists, laboratorians, environmental health staff, and public information teams.
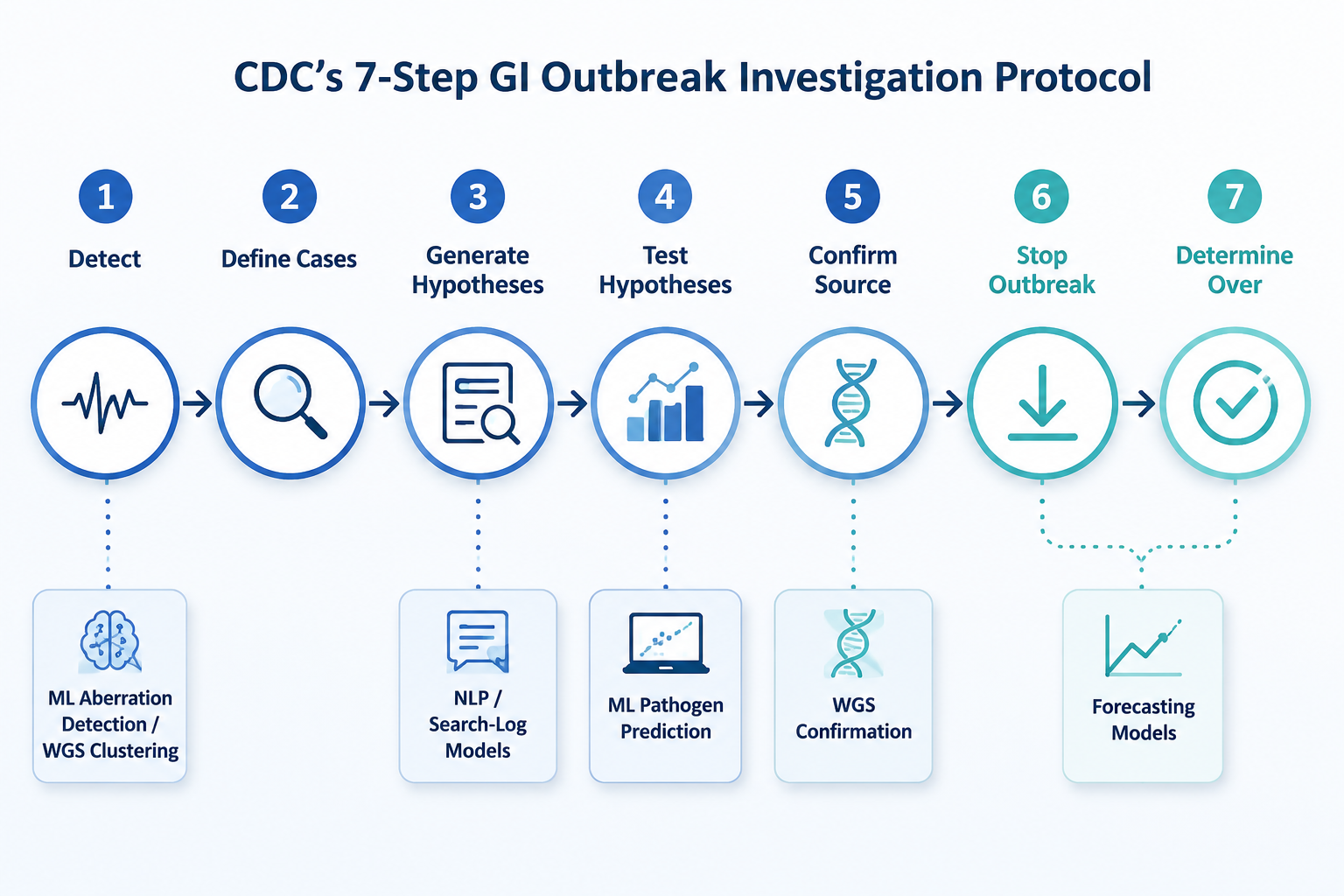
Where AI Sits In The Seven-Step Protocol
The useful map is not “AI versus traditional surveillance.” It is which analytic output belongs to which outbreak task. Some tools are already part of named public health infrastructure. Others are peer-reviewed demonstrations that show what could be useful, while leaving operational status or transferability unresolved.
| CDC protocol step | AI/ML or advanced analytic fit | What the output can help decide | What it cannot decide alone |
|---|---|---|---|
| 1. Detect a possible outbreak | NSSP/EARS aberration detection; PulseNet WGS clustering | Whether a symptom pattern or molecular cluster deserves review | Whether cases share a source or exposure |
| 2. Define and find cases | Structured surveillance queries; lab and WGS linkage | Which records and isolates should be pulled into the working line list | The final case definition without clinical, lab, time, place, and person review |
| 3. Generate hypotheses | Search-log models such as FINDER; NLP/social signal analysis; interview text support | Which restaurants, foods, places, or exposure categories should be examined sooner | Whether an exposure caused the outbreak |
| 4. Test hypotheses | ML pathogen prediction and analytic triage models | Which pathogen or hypothesis may deserve faster lab or epidemiologic follow-up | Source attribution, causality, or regulatory action |
| 5. Confirm source | PulseNet WGS comparison and cluster analysis | Whether isolates are genetically related enough to support a common-source investigation | The food vehicle without epidemiologic and traceback evidence |
| 6. Stop the outbreak | Forecasting models such as CIDMATH/Insight Net | Whether trajectory estimates should shape staffing, messaging, or intervention timing | Which control measure is sufficient without field evidence |
| 7. Determine whether it is over | Forecasting and surveillance trend models | Whether observed decline is consistent with expected outbreak behavior | Closure without continued surveillance and case ascertainment |
Detection Is Where Timing Matters Most
The strongest argument for AI in GI outbreak work begins before a source is visible. Traditional foodborne illness reporting can lag by weeks as a sick person seeks care, a specimen is collected, a laboratory result is produced, the result is reported, and enough related reports accumulate to look unusual. That 3–4 week reporting lag is the window in which digital signals are most tempting: emergency department syndromic data, search activity, geolocated complaints, and molecular clusters may surface before the complete epidemiologic picture exists.
CDC’s public AI program examples include the National Syndromic Surveillance Program using machine learning to analyze real-time emergency department symptom data for earlier GI outbreak signals.[3] That matters because syndromic surveillance is positioned at the front end of care-seeking, not after every laboratory and reporting step has finished. In practice, the model output is a cue for review: an aberration in vomiting, diarrhea, or related chief complaints may push an analyst to compare geography, age patterns, timing, and concurrent reports.
The evidence available from CDC’s AI program page is programmatic rather than granular. It supports that ML is being used in a real CDC surveillance context, but it does not provide the kind of sensitivity, specificity, false-alert rate, or site-level validation detail needed to compare performance cleanly against conventional aberration detection. That distinction is not a minor caveat. A tool can be deployed and still leave open how much it improves detection, where it performs best, and how often it sends investigators toward noise.
PulseNet sits differently in the evidence stack. The national laboratory network subtypes more than 75,000 isolates annually across nine tracked bacterial pathogens, and its transition to whole genome sequencing selected core genome and whole genome multilocus sequence typing for standardization and international harmonization.[4] CDC also describes WGS as a way to detect outbreaks by identifying bacterial isolates that are closely related genetically, which can connect illnesses that might otherwise look scattered across jurisdictions.[5]
For Step 1, WGS is not simply a better laboratory method; it changes the shape of the signal. A cluster may emerge because isolates match genetically, not because an interviewer has already found a shared restaurant or product. That can widen the first field of view, especially for multistate events where no single local health department sees enough cases to recognize the pattern.
The risk is over-reading the cluster. Closely related isolates make a common-source investigation more plausible; they do not name the source. The next move is still case definition, line-list review, patient interview, and exposure analysis. WGS improves the starting position, not the need for the investigation.
Defining Cases Still Controls The Rest Of The Work
AI receives less attention in Step 2 because the case definition is still a human epidemiologic construct. The team decides which clinical features, laboratory findings, time window, geography, and exposure criteria belong in the definition. A surveillance query or WGS cluster can help populate a working line list, but it cannot decide by itself whether a patient is confirmed, probable, possible, or outside the outbreak.
This is where a poorly placed model can do real damage. If an early digital signal is treated as the case definition, the investigation can become circular: the same pattern used to find the event becomes the pattern used to prove it. A better use is narrower. Use the model to find records, isolates, symptoms, or complaints that deserve review, then make the case definition explicit enough that another jurisdiction can apply it consistently.
Hypothesis Generation Is Broader Than Interviews Now
The classic hypothesis-generation task asks what cases have in common: foods eaten, places visited, events attended, water exposures, travel, animal contact, or contact with another sick person. Interviews remain central because they establish individual-level exposure histories. AI adds value here when it helps investigators decide what to ask about sooner, or where to send an environmental health team when the formal case count is still thin.
FINDER is the clearest peer-reviewed example of digital exhaust being used for this phase. The Google-led system used de-identified, aggregated search and location patterns to identify restaurants associated with possible foodborne illness. In the 2018 npj Digital Medicine study, the model reported a ROC AUC of 0.85 and F1 score of 0.74 across 15,000 evaluated queries.[6]
The operational result was more concrete than a classification metric. In Las Vegas and Chicago, restaurants identified by FINDER were 3.06 times more likely to be deemed unsafe on inspection than restaurants selected through baseline inspection processes, with a 95% confidence interval of 2.14–4.35.[6] That is the kind of lift that belongs in a public health discussion because it connects a model score to a field action: which restaurant gets inspected.
FINDER’s limits are equally important. The study used 2016–2017 data and was conducted by Google researchers; the available material does not establish current CDC operational deployment in 2026.[6] The narrow conclusion is that search-log and location-derived models can enrich hypothesis generation and inspection targeting under studied conditions. It is not evidence that CDC gastrointestinal outbreak investigation protocols now depend on FINDER, or that search behavior can replace interviews.
Social media and NLP sit in the same early-warning family, but with different weaknesses. A 2023 Foods study used geolocated tweets, CDC NORS data, and transformer-based models including BERTweet and RoBERTa; the dataset included 110,000 geolocated tweets, and the combined NORS-plus-Twitter model reported 0.82 accuracy.[7] The study also found that food category distribution in the social data correlated with CDC NORS data.[7]
That supports a cautious use case: social text can help surface candidate foods, locations, or complaint clusters for hypothesis generation. It does not prove that social media accurately represents the underlying population at risk. Posts are uneven by age, geography, platform use, and willingness to complain publicly. A spike in online chatter may be useful precisely because it is early and messy; it is not clean enough to serve as the denominator.
Testing A Hypothesis Is Not The Same As Predicting A Pathogen
Once a hypothesis exists, the protocol changes character. Investigators are no longer just widening the search. They are asking whether a suspected exposure explains illness better than alternatives. That can involve analytic epidemiology, laboratory testing, environmental assessment, product tracing, and comparison with background exposure patterns.
A JMIR study of gradient boosting decision tree models shows where ML may support this step without taking it over. Using Chinese foodborne disease surveillance data from 2011–2018, the model predicted four major pathogens — Salmonella, norovirus, E. coli, and Vibrio parahaemolyticus — with 69% accuracy without laboratory testing.[8]
For outbreak operations, that kind of model is best treated as triage. If symptoms, season, incubation pattern, and exposure features point toward a likely pathogen, a team may prioritize certain tests, interview modules, or control messages. But 69% accuracy also means a substantial share of predictions are wrong, and the study population and surveillance structure were Chinese rather than U.S. CDC data.[8] The finding should not be imported wholesale into U.S. practice without local validation.
The distinction matters because pathogen prediction can sound more decisive than it is. A probable-pathogen output can help choose the next question. It cannot confirm the food vehicle, establish traceback, or decide that an implicated establishment should be closed. In CDC’s protocol language, it belongs in the evidence-building phase, not at the end of it.
Source Confirmation Is Where WGS Has The Strongest Institutional Footing
PulseNet’s WGS transition is the most mature example in this article because it is not only a model demonstration. It is part of national molecular surveillance infrastructure. The 2019 Foodborne Pathogens and Disease review describes the move toward WGS standardization, the scale of annual isolate subtyping, and economic estimates from a 2016 analysis: approximately 270,000 illnesses prevented and more than $500 million saved annually, against an operating cost of $10–15 million.[4]
Those estimates should be read with date discipline. They come from an earlier economic analysis and may not reflect 2026 costs or savings. Still, they show why molecular cluster detection has become a central part of enteric outbreak investigation rather than a side experiment. WGS gives investigators a sharper way to ask whether cases that appear geographically separate may be part of the same event.
In Step 5, the most defensible wording is that WGS helps confirm relatedness among isolates and supports source confirmation when combined with epidemiologic and traceback evidence. It does not, by itself, prove that a specific lot, farm, restaurant, or food item caused illness. A tight genomic cluster can send investigators back to interviews with better focus; a matched food or environmental isolate can strengthen the case; but the source conclusion still depends on converging evidence.
Control And Closure Need Forecasts, Not Autopilots
The later steps of CDC gastrointestinal outbreak investigation protocols are less about discovering the signal and more about acting under uncertainty. Once a likely source is identified, teams may remove a product, close or correct a facility, issue public warnings, change infection-control practices, or continue surveillance while new cases are reported from earlier exposures.
CDC’s Insight Net material describes CIDMATH work using machine learning on Twitter/X data combined with clinical signals for norovirus outbreak trajectory prediction.[9] This is a plausible direction for Steps 6 and 7 because trajectory estimates can help with staffing, communications timing, and expectations about whether observed case counts are consistent with an outbreak slowing down.
The available CDC description does not provide full sensitivity and specificity detail for the Twitter/X-based norovirus forecasting approach.[9] That keeps the conclusion narrow. Forecasting can support situational awareness and planning; it is not a replacement for ongoing case ascertainment, nor does it decide that an outbreak is over. The decision still depends on the incubation period, reporting delays, exposure timing, pathogen characteristics, and continued surveillance.
CDC’s Center for Forecasting and Outbreak Analytics gives this work an institutional home for outbreak forecasting and analytic preparedness, but GI outbreak control remains a mixed operational problem: field teams need to know whether exposure has stopped, whether contaminated product remains available, whether new cases reflect old exposure, and whether public messaging is reaching the right people.[10]
Validated, Suggestive, And Out-Of-Scope Signals Should Not Be Blended
The evidence base is uneven in ways that matter for public health use. PulseNet WGS has national surveillance scale and standardization behind it. CDC’s NSSP machine-learning work has programmatic documentation but limited public performance detail. FINDER has unusually concrete inspection lift, but unclear 2026 operational status in CDC workflows. NLP and Twitter/X models show signal potential, but the available metrics do not make them equivalent to laboratory surveillance.
The pathogen prediction evidence is also narrower than it may first appear. A 69% model accuracy result from Chinese surveillance data is relevant to the general question of ML triage, but it is not a validation study for U.S. CDC outbreak response. Transferability would depend on reporting structures, pathogen prevalence, food patterns, clinical coding, laboratory practices, and the way missing data are handled.
Scope matters as well. The examples here mainly concern bacterial and viral GI outbreaks, especially foodborne and norovirus-relevant workflows. Parasitic enteric outbreaks, such as Cyclospora or Cryptosporidium, can follow related surveillance and interview logic but often require distinct laboratory, exposure, and environmental pathways. For that narrower clinical lane, ClinicalMind’s cyclosporiasis outbreak overview is a better fit than treating all GI outbreak protocols as interchangeable.
What AI Actually Changes In CDC GI Outbreak Work
AI’s practical contribution is not a new protocol. It is a change in timing, linkage, and prioritization inside the existing one. NSSP-style syndromic models can push a symptom signal forward. Search-log and NLP systems can suggest candidate exposures before interviews have converged. WGS can connect cases across jurisdictions with more precision than older subtyping. Pathogen prediction can help triage testing and analytic attention. Forecasting can help teams plan while surveillance is still incomplete.
The decisive framework remains epidemiological investigation. Someone still has to decide who counts as a case, ask patients what they ate and where they went, reconcile laboratory and exposure data, test the suspected association, assess environmental evidence, and decide whether action is justified. The strongest AI tools in CDC gastrointestinal outbreak investigation protocols are the ones that respect that sequence rather than pretending to replace it.
References
- Acute Enteric Disease Outbreaks, CDC Field Epidemiology Manual.
- Steps in a Foodborne Outbreak Investigation, CDC.
- Examples of CDC Programs Currently Using AI, CDC.
- Transforming Local, National, and International Public Health Surveillance for Foodborne Pathogens Using Whole Genome Sequencing, Foodborne Pathogens and Disease, 2019.
- Detecting Outbreaks with Whole Genome Sequencing, CDC.
- Machine-learned epidemiology: real-time detection of foodborne illness at scale, npj Digital Medicine, 2018.
- Foodborne Illness Detection Using Social Media, Foods, 2023.
- A Machine Learning Model for Predicting the Etiology of Foodborne Disease Outbreaks, JMIR, 2021.
- AI and Machine Learning, CDC Insight Net.
- Center for Forecasting and Outbreak Analytics, CDC.
Comments
Join the discussion with an anonymous comment.