The most clinically important shift in the wildfire smoke health effects discussion is not that wildfire smoke raises PM2.5. It is that a microgram of wildfire-derived PM2.5 may not behave like a microgram of conventional fossil-fuel-derived ambient PM2.5. Stanford researchers Patel and Burke summarized multiple toxicological and epidemiological lines of evidence indicating that wildfire PM2.5 is approximately 10 times more toxic per μg/m³ than PM2.5 from fossil-fuel combustion.[1]
That estimate should be read carefully. It is not a single randomized comparison, and wildfire exposure cannot be assigned or measured at every doorstep with trial-like precision. The claim rests on converging evidence: wildfire particles can be smaller, can carry higher concentrations of oxidative and pro-inflammatory compounds, and are produced under combustion conditions that differ from routine urban fossil-fuel emissions.[1] For clinicians and public health researchers, the practical implication is still substantial: conventional PM2.5 assumptions may understate risk during smoke episodes.

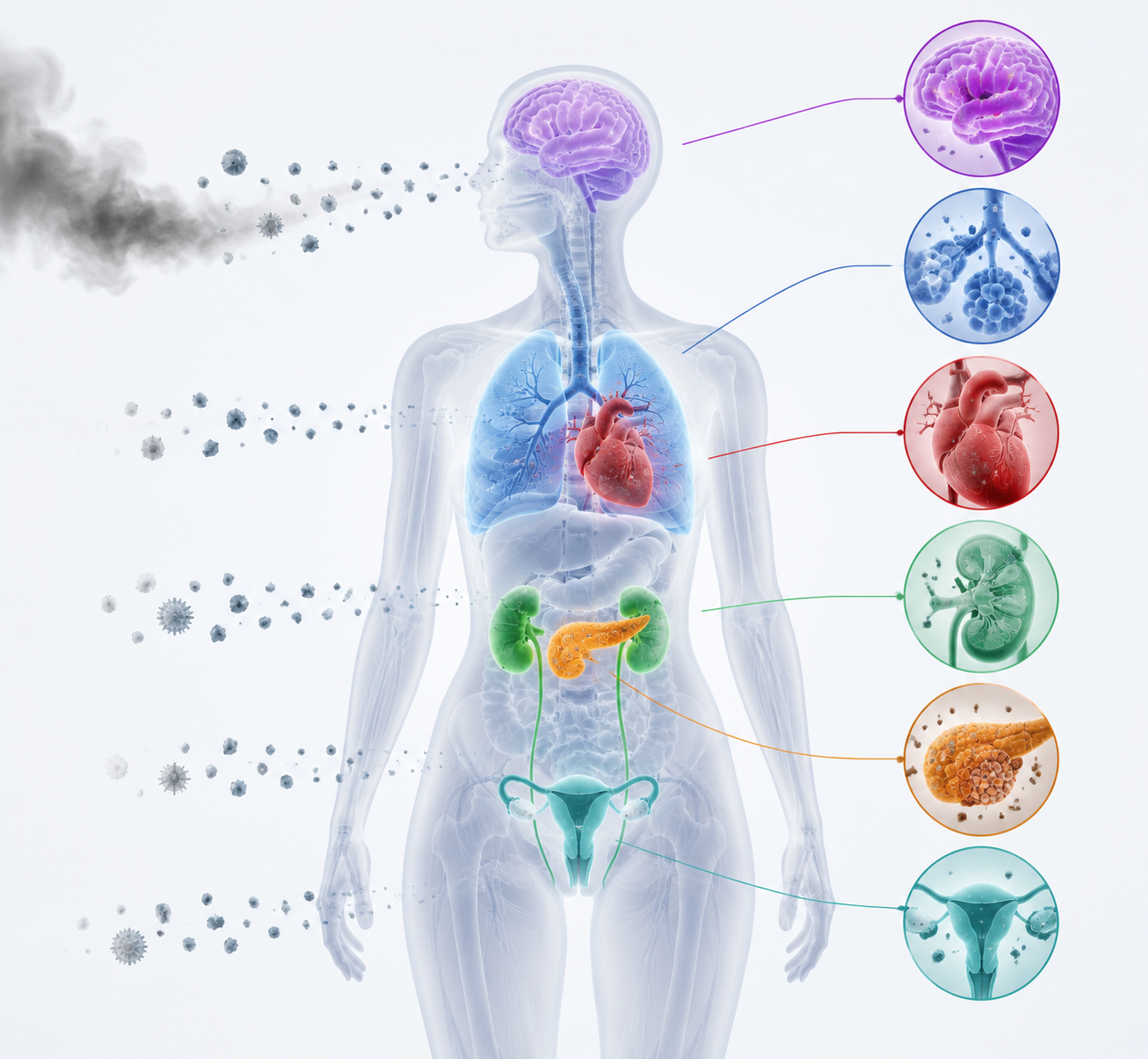
This matters because the downstream signal is no longer confined to cough, wheeze, or emergency inhaler use. The strongest evidence still sits in respiratory and cardiovascular outcomes, where large hospitalization datasets can detect short-term changes. But the current literature also includes national mortality estimates, dementia associations, and emerging endocrine, renal, and reproductive findings. The clinical task is not to pretend the evidence is equally mature across every organ system. It is to recognize that wildfire smoke is now showing up across enough endpoints, populations, and time windows that treating it as a temporary air-quality nuisance is no longer defensible.
Why Wildfire PM2.5 Is Not Just More PM2.5
PM2.5 is a mass-based measure: particles with aerodynamic diameter of 2.5 micrometers or smaller. That measurement is useful because small particles can penetrate deeply into the respiratory tract and contribute to systemic inflammation. But mass alone does not describe composition, oxidative potential, surface chemistry, or the combustion source that produced the particles.
The Stanford synthesis is important because it challenges a common shortcut: reading wildfire smoke through the same risk lens used for everyday ambient PM2.5. Patel and Burke describe wildfire PM2.5 as approximately 10 times more toxic per unit mass than fossil-fuel PM2.5, with plausible mechanisms including smaller particle size, more oxidative and inflammatory chemical profiles, and combustion conditions that can generate different toxic constituents.[1] The estimate is deliberately broad, but it is not casual. It combines mechanistic plausibility with epidemiological signals that repeatedly find stronger health associations for wildfire-specific PM2.5 than for non-wildfire PM2.5.
The distinction is not academic. A clinician looking at a modest smoke-related increase in PM2.5 may underestimate population risk if the exposure is interpreted as interchangeable with traffic or industrial PM2.5. Conversely, an editor or researcher should not flatten the 10× estimate into a universal constant that applies to every fire, fuel type, and exposed community. Wildfire smoke composition changes with vegetation, structures burned, atmospheric aging, and meteorology. The current evidence supports a directional judgment: wildfire PM2.5 can be substantially more harmful per unit mass than conventional ambient PM2.5, and that difference should shape how health effects are interpreted.
Respiratory Evidence: The Clearest Acute Signal
Respiratory outcomes remain the most direct place to see wildfire smoke move from air monitoring into clinical burden. Aguilera and colleagues analyzed Southern California data and compared wildfire-specific PM2.5 with PM2.5 from non-wildfire sources. They reported a 1.3% to 10% increase in respiratory hospitalizations per 10 μg/m³ increase in wildfire PM2.5, compared with about 1% for PM2.5 from non-wildfire sources.[2]
That comparison does two things well. First, it avoids treating all fine particles as equivalent simply because they share a size category. Second, it anchors the toxicity discussion in observed healthcare use rather than only in laboratory plausibility. Hospitalization is an imperfect endpoint, because it misses symptoms managed at home, outpatient visits, missed work, and people who avoid care. But as a severe endpoint, it is hard to dismiss. Someone crossed a threshold where home management, outpatient advice, or delayed care was no longer enough.
The Southern California setting also deserves a plain reading. It is not the entire United States, and several major wildfire health studies draw on California or western U.S. exposure patterns. That overlap is a replication constraint, not a reason to ignore the findings. California has enough repeated smoke exposure, dense population, health system data, and monitoring infrastructure to make certain analyses possible. The more precise question is whether the same magnitude of association appears in other regions, age distributions, housing conditions, and healthcare access environments.
Cardiorespiratory Risk Can Outlast the Fire
A smoke plume disappears from the skyline before every physiologic process it triggered has resolved. Wei and colleagues examined 13.8 million cardiovascular and 8 million respiratory hospitalizations across 15 U.S. states and found that elevated cardiorespiratory risks, including ischemic heart disease, hypertension, COPD, and pneumonia, could persist up to three months after fires ended.[3]
The time window is clinically consequential. If risk remains elevated after the visible event, surveillance that ends when the smoke clears will miss part of the burden. Emergency departments may see acute exacerbations during the episode; primary care, cardiology, pulmonology, and public health offices may inherit the tail. This is also where patient-level advice alone becomes too narrow a frame. A three-month elevation in risk is a system signal: medication access, follow-up capacity, hospitalization monitoring, and public health messaging all sit downstream of the exposure.
| Evidence Area | What the cited study measured | Clinical reading |
|---|---|---|
| Respiratory admissions | 1.3% to 10% increase in respiratory hospitalizations per 10 μg/m³ wildfire PM2.5 in Southern California | Strong acute signal; wildfire PM2.5 appears more harmful than non-wildfire PM2.5 for respiratory admissions |
| Cardiorespiratory persistence | 13.8 million cardiovascular and 8 million respiratory hospitalizations across 15 states | Risk can remain elevated up to three months after fires end |
| Long-term mortality | All 3,108 U.S. counties from 2006 to 2019 | Wildfire PM2.5 contributes to national annual excess mortality, not only episodic symptoms |
| Dementia | 1.2 million Kaiser Permanente Southern California members | Neurological associations are substantial but still need careful interpretation |
Long-Term Mortality: The Denominator Is the Country
The heaviest quantitative burden in the current evidence base comes from Ma and colleagues’ PNAS analysis of long-term wildfire smoke PM2.5 exposure and mortality across all 3,108 counties in the contiguous United States from 2006 through 2019.[4] The study estimated approximately 11,415 excess nonaccidental deaths per year attributable to long-term wildfire smoke PM2.5 exposure.[4]
The cause-specific estimates are especially relevant for clinicians who might otherwise confine wildfire smoke to pulmonary medicine. Ma et al. estimated about 4,512 cardiovascular deaths, 1,142 endocrine and diabetes-related deaths, and 320 chronic kidney disease deaths per year attributable to long-term wildfire smoke PM2.5 exposure.[4] Those categories do not make wildfire smoke the sole cause of the deaths; they estimate excess mortality associated with the modeled exposure in the population. The distinction matters. Attribution in this setting is statistical and population-level, not a bedside declaration that smoke caused an individual death.
The national county-level design gives the study weight because it moves beyond a single fire season or single metropolitan area. It also depends on exposure modeling. Long-term wildfire PM2.5 cannot be reconstructed by asking every person where they were, whether their windows were sealed, whether they used filtration, or how much time they spent outdoors. Researchers therefore rely on satellite-derived PM2.5, smoke identification, ground monitoring, and chemical transport models to estimate exposure over space and time. Those methods are necessary at national scale. They are also least able to see the exact differences that often matter to patients: indoor infiltration, occupational exposure, neighborhood-level smoke pooling, housing quality, and individual behavior during smoke days.
This is the recurring tension in wildfire epidemiology. The better the study covers a population, the less it can know about every person’s actual inhaled dose. The right response is not to discard modeled evidence. It is to keep the inference at the level the methods support: long-term wildfire smoke PM2.5 is associated with measurable excess mortality at national scale, while individual exposure misclassification remains a serious limitation.
Neurological Findings: A Dementia Signal That Should Not Be Overread or Ignored
The neurological evidence is less mature than the respiratory and cardiovascular evidence, but the dementia findings are no longer a marginal curiosity. Elser and colleagues analyzed a Kaiser Permanente Southern California cohort of 1.2 million members and found that each 1 μg/m³ increase in three-year mean wildfire PM2.5 was associated with an 18% increase in dementia odds. The corresponding increase for non-wildfire PM2.5 was 1%.[5]
The contrast between wildfire and non-wildfire PM2.5 is again the most important feature. A unit increase in mass did not carry the same association across sources. That pattern is consistent with the broader toxicity argument, although it does not by itself prove a specific biological pathway from wildfire smoke to dementia. Dementia risk is shaped by age, vascular disease, socioeconomic factors, baseline health, healthcare access, diagnostic practices, and many other exposures. A cohort study can adjust for measured confounders; it cannot make smoke exposure randomized.
The Kaiser cohort also reinforces the geography issue. Southern California is not incidental to the study; it is part of why the analysis is possible. The finding should therefore be treated as a strong signal in a large insured population with meaningful wildfire exposure, not as final proof that the same effect size applies everywhere. Still, an 18% increase in dementia odds per 1 μg/m³ three-year mean wildfire PM2.5 is too large to leave outside clinical awareness, particularly because cardiovascular and inflammatory pathways already connect air pollution to brain health hypotheses.[5]
Endocrine, Renal, and Reproductive Signals
The endocrine and renal findings currently sit in a different evidentiary position from respiratory admissions. They are important, but they are not yet supported by the same breadth of endpoint-specific literature. Ma et al. nevertheless gives these systems a population-level mortality signal: approximately 1,142 endocrine and diabetes-related deaths and 320 chronic kidney disease deaths per year were attributed to long-term wildfire smoke PM2.5 exposure in the contiguous United States.[4]
Those estimates should widen clinical attention without overstating mechanism. Diabetes and kidney disease are chronic conditions with complex causal pathways. The mortality analysis indicates that wildfire smoke PM2.5 contributes to excess deaths in these categories at population scale. It does not tell a clinician exactly which patient with diabetes will decompensate after a smoke season, or whether the relevant pathway is inflammatory stress, cardiovascular worsening, medication disruption, reduced outdoor activity, infection susceptibility, or some combination.
Reproductive evidence is also emerging. CU Boulder’s summary of Reid and colleagues’ work reports associations between gestational wildfire smoke exposure and lower birth weight and preterm birth.[6] These outcomes matter because small shifts across many pregnancies can become visible at the population level even when any one pregnancy has multiple risk factors. But the evidence should not be made to carry the same weight as the hospitalization literature. The most careful interpretation is that pregnancy is a plausible and increasingly documented vulnerability window, with observed associations for birth weight and preterm birth that warrant obstetric and public health attention.
What Exposure Models Can See, and What They Miss
The best wildfire smoke studies depend on exposure models because the alternative is not perfect measurement. It is no measurement at the scale needed. Satellite-derived PM2.5 helps reconstruct smoke over wide regions. Chemical transport models estimate how emissions move and transform through the atmosphere. Ground monitors help anchor modeled concentrations to observed air quality. Together, these tools allow researchers to analyze all U.S. counties, millions of hospitalizations, or a 1.2 million-member health system cohort.
The blind spots are clinically familiar. Outdoor modeled PM2.5 does not equal inhaled dose. Two people in the same census tract may have different exposure because one works outdoors, one uses high-efficiency filtration, one lives in leaky housing, one has access to clean indoor air, and one evacuates temporarily. Within-community variation can be large, and indoor exposure is often poorly captured. These limitations usually bias studies toward uncertainty, not toward bedside specificity.
This is why the comparison between wildfire and non-wildfire PM2.5 is so useful. It asks whether particles assigned to wildfire sources show stronger associations than particles from other sources within the same broad PM2.5 framework. Aguilera et al. found a larger respiratory hospitalization association for wildfire PM2.5 than for non-wildfire PM2.5.[2] Elser et al. found a much larger dementia association for wildfire PM2.5 than for non-wildfire PM2.5.[5] These are not interchangeable endpoints, but the pattern is hard to square with a generic “PM2.5 is PM2.5” assumption.
The Clinical Reading of the Evidence
The strongest current evidence supports three clinical conclusions. First, wildfire smoke PM2.5 has acute respiratory and cardiovascular effects that appear in hospitalization data. Second, the risk window can extend beyond the visible smoke episode, with cardiorespiratory elevations reported up to three months after fires end.[3] Third, longer-duration exposure is associated with national excess mortality and with signals in neurological, endocrine, renal, and reproductive outcomes.[4][5][6]
The evidence is not uniform. Respiratory and cardiovascular outcomes are the most developed, supported by large acute-care datasets and source-specific PM2.5 comparisons. Dementia evidence is substantial but still concentrated in a large Southern California cohort. Endocrine, renal, and reproductive findings are clinically important but newer and less densely replicated. Population studies rely on modeled exposure, and those models cannot fully resolve indoor dose, neighborhood variation, or individual protective conditions.
Those caveats narrow the claim; they do not erase it. Wildfire smoke PM2.5 is a multi-system exposure with measurable associations across respiratory, cardiovascular, neurological, endocrine, reproductive, and renal outcomes. Its effects can outlast the fire event. And if wildfire PM2.5 is approximately 10 times more toxic per unit mass than fossil-fuel PM2.5, then a familiar air-quality metric may be understating the clinical stakes during smoke seasons.[1]
For readers focused on prediction methods, ClinicalMind’s related review of AI wildfire smoke health prediction examines how machine learning is being used to anticipate health impacts. The epidemiological synthesis here is more basic and more urgent: the evidence is strong enough to warrant clinician and public health attention now, even while exposure models improve and organ-specific evidence continues to mature.
References
- Assessing wildfire health risks. Stanford News. 2025.
- Fine particles in wildfire smoke and pediatric respiratory health in California. Nature Communications. 2021.
- Cardiorespiratory effects of wildfire smoke particles can persist for months, even after a fire has ended. Harvard T.H. Chan School of Public Health. 2025.
- Long-term exposure to wildland fire smoke PM2.5 and mortality in the contiguous United States. PNAS. 2024.
- Wildfire Smoke Exposure and Incident Dementia. JAMA Neurology. 2024.
- Wildfire smoke is bad for your health. CU Boulder Today. 2026.
Comments
Join the discussion with an anonymous comment.