Introduction: The $1.3 Trillion Administrative Cost Problem
In 2024, total U.S. healthcare spending reached $5.3 trillion. Of that, roughly 25% — approximately $1.3 trillion — went to administrative functions, not clinical care. That figure, cited by the American Hospital Association (AHA) and drawn from a JAMA analysis, captures the full cost of billing, coding, prior authorization, claims processing, scheduling, and documentation. For context, $1.3 trillion exceeds the entire GDP of most countries. It is the price the system pays for complexity.
For health system administrators, CFOs, and revenue cycle directors, this number is not abstract. It shows up in denial rates that average 10–15% of claims, in the 19 hours per week physicians spend on administrative tasks, and in the burnout statistics that have become a workforce crisis. The question is no longer whether artificial intelligence can help. It is whether the current generation of deployed AI tools delivers measurable, repeatable returns that justify the investment.
This article surveys the evidence across the three administrative domains where AI has moved beyond pilots into production: revenue cycle management and billing, prior authorization automation, and ambient documentation. The benchmarks that follow come from peer-reviewed studies, industry surveys, and published deployment data — not vendor white papers. The goal is to give decision-makers a grounded, evidence-based reference for evaluating AI tools in 2026.
Adoption Landscape: From Pilots to Deployed Systems
The adoption curve for administrative AI has steepened markedly over the past two years. According to McKinsey's Q4 2024 survey, 85% of healthcare leaders are either exploring or have already adopted generative AI in some capacity. More importantly, 64% of those who have implemented AI solutions report positive ROI. That figure represents a significant shift from earlier years when pilot programs struggled to demonstrate clear financial returns.
A 2025 AHA survey identified billing and scheduling as the two fastest-growing AI use cases across U.S. hospitals. This aligns with broader market data: U.S. healthcare AI spending nearly tripled to $1.4 billion in 2025, and the global generative AI in healthcare market — valued at approximately $800 million in 2022 — is projected to reach $17.2 billion by 2032, according to Market.us.
However, adoption is not uniform. A HIMSS survey found that while 85% of organizations have explored AI, only 18% are actually ready to deploy it in care delivery settings. The gap between exploration and production readiness is particularly wide in administrative workflows, where legacy EHR integration and data quality issues create friction. The table below summarizes the current state across the three main administrative domains.
| Domain | Adoption Signal | Key Benchmark | Source |
|---|---|---|---|
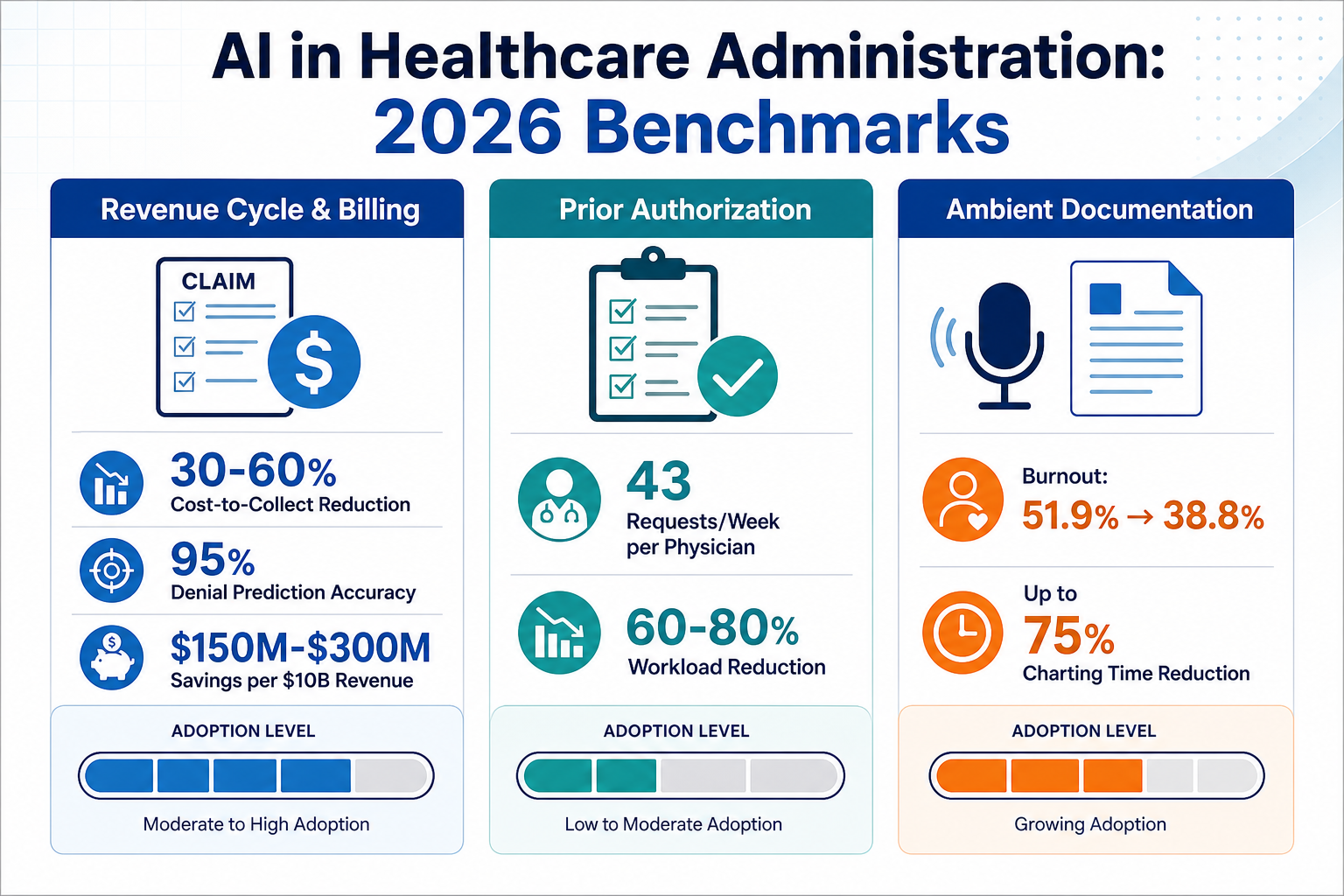
| Revenue Cycle & Billing | Fastest-growing AI use case per AHA 2025 survey | 30–60% cost-to-collect reduction | McKinsey 2024–2025 |
| Prior Authorization | 43 requests/week per physician; ~12 staff hours per cycle | 60–80% workload reduction on straightforward cases | AMA 2024–2025 |
| Ambient Documentation | Gartner calls ambient scribes a 'likely win' for health systems | Burnout drop from 51.9% to 38.8% after 30 days | JAMA Network Open 2025 |

The shift from pilots to deployed systems is also reflected in investment patterns. In 2025, 54% of all digital health funding went to AI-enabled companies, according to Rock Health. EHR vendors including Epic and Oracle Health are increasingly embedding AI capabilities directly into their platforms, which both accelerates adoption and creates competitive pressure for standalone AI vendors.
Revenue Cycle and Billing AI: Measurable ROI and Accuracy Gains
Revenue cycle management (RCM) is the domain where AI has produced the most concrete, auditable ROI figures. The reason is straightforward: RCM involves high-volume, rules-based processes — claim submission, denial management, coding, payment posting — that are well-suited to pattern recognition and automation. Unlike clinical AI, where outcomes are measured in sensitivity and specificity, RCM AI is measured in dollars recovered, days in accounts receivable, and denial rates.
McKinsey's 2024–2025 analysis found that AI-enabled RCM reduces cost to collect by 30–60%. For a health system with $10 billion in annual payer revenue, that translates to $150 million to $300 million in savings. These are not theoretical projections — they are based on deployed systems at scale.
| Metric | Benchmark | Source |
|---|---|---|
| Cost-to-collect reduction | 30–60% | McKinsey 2024–2025 |
| Savings per $10B revenue | $150M–$300M | McKinsey 2024–2025 |
| Claim denial prediction accuracy | 95% | Keragon / RapidClaims 2025–2026 |
| Hybrid AI-human first-pass coding rate | 95%+ | HOMRCM 2025 |
| Denial rate reduction | 40–50% | HOMRCM 2025 |
| Time saved for revenue cycle professionals | 41–50% across all stages | Deloitte |
The 95% claim denial prediction accuracy figure comes from tools that analyze historical claims data, payer policies, and clinical documentation to flag claims likely to be denied before submission. This predictive capability shifts denial management from a reactive process — appealing denials after they occur — to a preventive one. Given that $262 billion in medical claims are initially denied industry-wide, with 86–90% considered avoidable according to the AHA, even modest improvements in prediction accuracy have substantial financial impact.
Hybrid AI-human coding models represent another high-impact use case. Rather than replacing coders, these systems use AI to generate initial code suggestions based on clinical documentation, which human coders then review and refine. The result is first-pass accuracy rates above 95%, compared to industry averages that often fall below 80% for fully manual processes. Denial rates drop by 40–50% because the coding is more complete and specific from the start.
A Deloitte study found that generative AI can save between 41% and 50% of the time spent by revenue cycle professionals across all stages of the RCM workflow. This time savings compounds: faster coding means faster claim submission, which reduces days in accounts receivable and improves cash flow. For health systems operating on thin margins — many of which saw operating margins below 2% in 2024 — these improvements are material.
Prior Authorization Automation: Workload Reduction at Scale
Prior authorization remains one of the most burdensome administrative processes in U.S. healthcare. According to AMA data, the average physician handles 43 prior authorization requests per week, and each request consumes approximately 12 staff hours across the full cycle — from initial submission to appeal. 93% of physicians report that prior authorization delays patient care.
AI-based prior authorization tools address this bottleneck by automating the initial triage and documentation gathering stages. For straightforward cases — those that match established clinical criteria and require no additional clinical judgment — AI routing can reduce staff workload by 60–80%. The system extracts relevant information from the EHR, maps it to payer-specific criteria, and generates a pre-populated submission packet that a human reviewer can approve with minimal additional effort.
| Metric | Value | Source |
|---|---|---|
| Prior auth requests per physician per week | 43 | AMA 2024–2025 |
| Staff hours per prior auth cycle | ~12 | AMA 2024–2025 |
| Physicians reporting care delays due to prior auth | 93% | AMA |
| AI workload reduction on straightforward cases | 60–80% | Industry benchmarks |
| Physician time spent on admin tasks per week | Up to 19 hours | AMA |
It is important to distinguish between the current generation of AI prior authorization tools — which primarily automate information gathering and routing — and the more ambitious vision of fully automated clinical appropriateness assessment. The latter, as proposed in a 2023 JAMIA perspective by Lenert et al., would use deep learning transformer models fine-tuned on expert panel consensus to simulate appropriateness determinations. That approach remains conceptual; deployed systems today focus on workflow efficiency rather than clinical judgment.
Ambient Documentation and AI Scribes: Burnout Reduction and Time Savings
Ambient clinical intelligence — AI scribes that listen to patient encounters and generate clinical notes in real time — has emerged as one of the most impactful administrative AI applications, not because it saves the most money, but because it directly addresses the clinician burnout crisis. Physician burnout, which costs the U.S. economy approximately $4.6 billion annually, is driven in large part by documentation burden. Physicians spend up to 19 hours per week on administrative tasks, much of it on charting.
The strongest evidence comes from a 2025 study published in JAMA Network Open. Researchers found that clinician burnout dropped from 51.9% to 38.8% after 30 days of ambient AI scribe use — a 13.1 percentage point reduction. Mass General Brigham reported an even larger effect: a 21.2 percentage point reduction in burnout with AI scribe deployment. These are not marginal improvements; they represent a meaningful shift in the clinician experience.
| Metric | Value | Source |
|---|---|---|
| Burnout rate before AI scribe use | 51.9% | JAMA Network Open 2025 |
| Burnout rate after 30 days of AI scribe use | 38.8% | JAMA Network Open 2025 |
| Burnout reduction (Mass General Brigham) | 21.2 percentage points | PMC 2024–2025 |
| Charting time reduction | Up to 75% | Industry benchmarks |
| Additional appointment hours per day (AHA estimate) | Up to 4 | AHA |
| Overall physician burnout rate (2025) | 41.9% | Medscape / Barton Associates |
The charting time reduction — up to 75% — translates directly into operational capacity. The AHA estimates that practices using ambient scribes gain up to four additional appointment hours per day because clinicians spend less time on documentation. For health systems facing primary care access shortages, this capacity gain is as valuable as the burnout reduction.
Gartner's research, cited in HealthTech Magazine, calls ambient scribes a "likely win" for health systems, noting improvements in coding accuracy, reimbursement capture, and clinician recruitment. The recruitment angle is often overlooked: health systems that offer ambient AI scribes as a standard tool report higher clinician satisfaction and retention, which reduces the substantial cost of locum tenens coverage and recruitment fees.
Implementation Barriers: Interoperability, Shadow AI, and Governance
The ROI benchmarks presented above are real, but they are not automatic. Health systems that fail to address three structural barriers — interoperability, shadow AI, and governance — will see significantly lower returns, and in some cases, negative outcomes.
Legacy EHR Integration
Most administrative AI tools require deep integration with the EHR to function effectively. Yet many health systems operate on legacy platforms with limited API capabilities. A 2024 Cureus review notes that interoperability remains a primary challenge, with many institutions running diverse systems that do not communicate seamlessly. The ONC's TEFCA framework and FHIR standards are gradually improving this landscape, but the transition is slow.
For health systems evaluating AI tools, integration readiness should be a first-order criterion — not an afterthought. Tools that require manual data exports or duplicate data entry will erode the efficiency gains they promise.
Shadow AI and Security Risks
Shadow AI — the use of unauthorized AI tools by staff — is present in 40% of hospitals, according to a 2026 Wolters Kluwer survey. 57% of healthcare professionals have used unauthorized AI tools, adding an average of $670,000 to breach costs per incident, per IBM's 2025 data breach report. When clinicians or administrative staff use consumer-grade AI tools for tasks like drafting prior authorization letters or summarizing patient histories, they expose the organization to HIPAA violations and data leakage.
The solution is not to ban AI use — that approach has already failed — but to provide approved, secure tools that meet the needs driving shadow AI adoption in the first place. This requires a governance framework that includes approved tool lists, staff training, and monitoring.
Human-in-the-Loop Models
Every successful administrative AI deployment documented in the literature uses a human-in-the-loop model. AI handles the high-volume, low-judgment tasks — routing prior authorization requests, flagging likely claim denials, generating draft clinical notes — but a human reviews, approves, or corrects the output before it becomes part of the permanent record. Full autonomy, particularly in billing and coding, carries unacceptable compliance risk.
This is not a limitation of the technology; it is a design choice that reflects the regulatory environment and the high cost of errors. A miscoded claim can trigger an audit, a repayment demand, or worse. A prior authorization denial based on an AI misinterpretation can delay patient care. Human oversight is not a workaround — it is a feature of responsible deployment.
Outlook and Recommendations for Health System Decision-Makers
The evidence surveyed in this article supports a clear conclusion: AI in healthcare administration has moved beyond the pilot phase and is delivering measurable, repeatable returns in revenue cycle management, prior authorization, and ambient documentation. The benchmarks — 30–60% cost-to-collect reduction, 95% denial prediction accuracy, 13+ percentage point burnout reduction — are not hypothetical. They come from deployed systems at scale.
However, these returns are contingent on implementation discipline. Based on the evidence reviewed, the following recommendations emerge for health system decision-makers:
- Prioritize high-ROI domains first. Revenue cycle management and ambient documentation have the strongest evidence bases and the most predictable returns. Start there before expanding into more experimental applications.
- Invest in interoperability infrastructure before purchasing AI tools. The best AI model is useless if it cannot access the data it needs. FHIR-enabled APIs and TEFCA compliance should be prerequisites, not nice-to-haves.
- Adopt human-in-the-loop models as the default. Full autonomy in billing, coding, and clinical documentation carries compliance and safety risks that outweigh the marginal efficiency gains.
- Establish a governance framework that addresses shadow AI. Provide approved tools, train staff, and monitor usage. The goal is to channel AI use into safe, auditable channels — not to suppress it.
- Monitor the evolving regulatory landscape. Nearly 40 states adopted or enacted around 100 AI-related measures in 2025, and the federal regulatory environment remains fragmented. Compliance requirements will continue to evolve.
- Request site-specific validation data from vendors. Industry benchmarks are useful for initial screening, but every health system has unique payer mix, patient population, and workflow characteristics. Insist on data from deployments similar to your own.
For a broader view of the evidence and policy context across both clinical and administrative AI, see the site's comprehensive overview: Generative AI in Healthcare: State of the Evidence and Policy Landscape in 2026. For market-level context on investment and adoption trends, see Health Tech AI in 2026: Where Investment, Adoption, and ROI Data Converge — and Where the Gaps Remain.