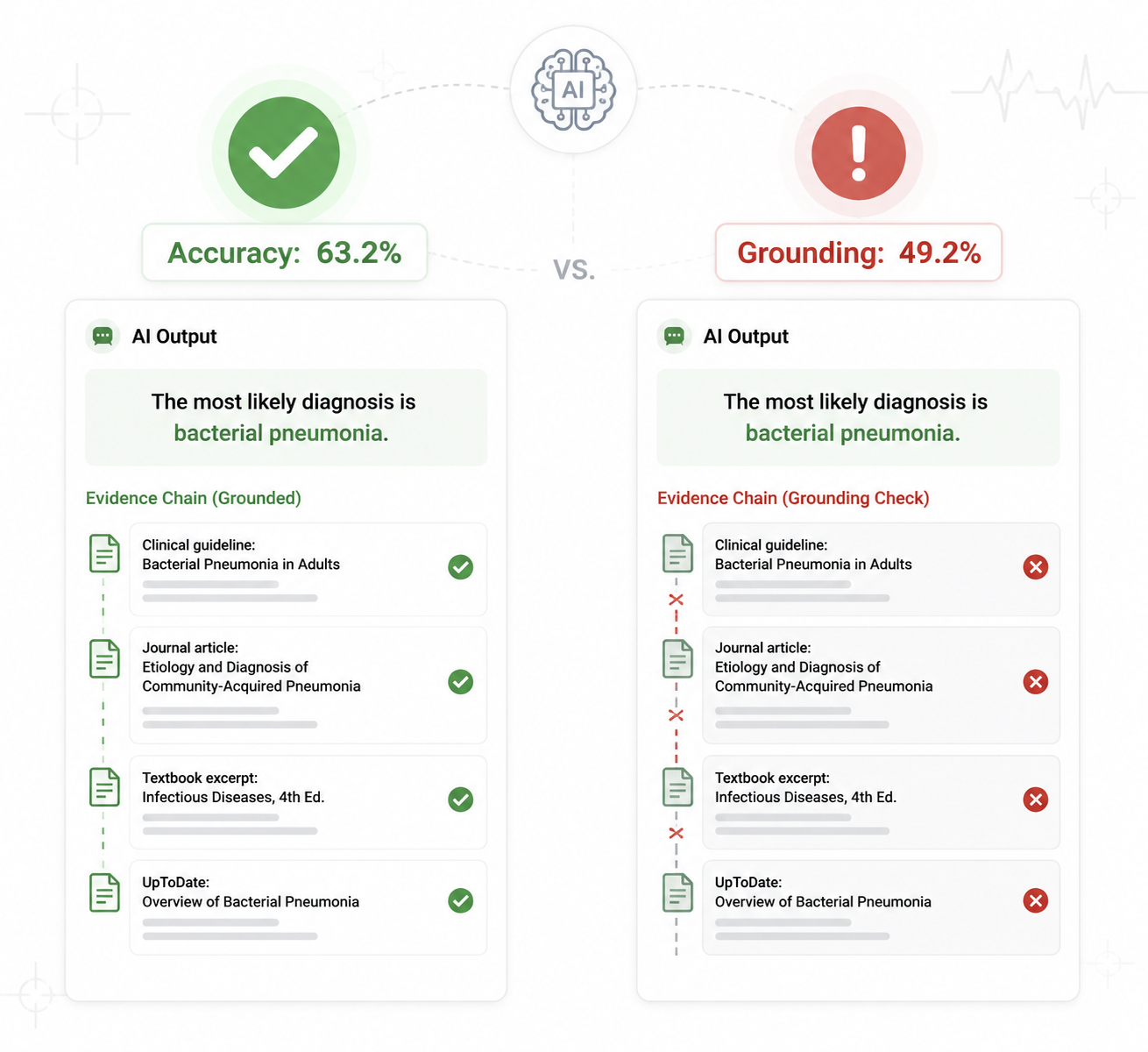
A medical RAG system can look reassuringly competent when the scorecard asks only one question: did the final answer match the benchmark label? In the RAG-X evaluation, the best-performing pipeline on MedQA reached 63.2% accuracy, but only 49.2% evidence-based grounding. More uncomfortable still, 33.9% of answers that looked correct were classified as “lucky guesses”: the retrieval step had failed, yet the generator still produced the right answer from its own parametric memory or prior exposure rather than from the retrieved evidence.[1]
That is the accounting problem at the center of medical RAG system validation. A correct answer is not automatically a grounded answer. If the retriever brought back weak or irrelevant context and the model answered correctly anyway, ordinary accuracy treats the run as a success. The clinical informaticist later asked to defend the system does not have that luxury. They need to know whether the answer was supported, whether the context was sufficient, and whether the model merely appeared to use evidence.
Retrieval-augmented generation is attractive in medicine precisely because it promises an evidence trail. The model should not simply pronounce; it should retrieve, condition, answer, and point back to the material that justified the response. But if validation rewards the final answer while ignoring whether the retrieved material carried the reasoning, the traceability promise becomes decorative. The system may be accurate on paper and still unreliable in the way that matters for clinical review.
What the Accuracy Score Failed to Count
RAG-X is useful because it does not stop at asking whether the final answer is right. It separates answer correctness from evidence use. That distinction sounds almost too obvious until one looks at how many benchmark tables collapse both into a single success column.
In the reported MedQA experiment, the 14-percentage-point difference between 63.2% accuracy and 49.2% grounding was not a rounding error. It represented cases where the answer-level metric credited outputs that the evidence chain did not justify.[1] For a general QA leaderboard, that may be a tolerable abstraction. For a medical RAG system, it is a validation blind spot.
The boundary matters because RAG systems can fail in more than one place. Retrieval can fail by returning irrelevant, incomplete, redundant, or misleading documents. Generation can fail by ignoring useful context. The model can also succeed for the wrong reason, drawing on memorized associations while the retrieved evidence sits beside the answer like an alibi. A final-answer accuracy metric cannot tell those cases apart.
| Validation question | What ordinary accuracy can see | What grounding-aware validation must see |
|---|---|---|
| Is the final answer correct? | Yes or no | Yes or no |
| Was the retrieved evidence relevant? | Usually invisible | Measured directly through context relevance or retrieval diagnostics |
| Was the retrieved evidence sufficient? | Usually invisible | Tested through sufficiency and insufficient-information scenarios |
| Did the generator actually use the evidence? | Usually invisible | Assessed through grounding, faithfulness, or context utilization metrics |
| Did the system succeed for the wrong reason? | Counted as success | Flagged as a lucky guess or related failure mode |
This is why the RAG-X result should not be read as a generic claim that all medical RAG systems have the same failure rate. The reported figures come from a best-performing pipeline on MedQA, not from every clinical specialty, base model, retriever, corpus, or workflow. The important contribution is diagnostic: it shows that a respectable answer score can hide a materially different evidence-use score.
The Four Cases a Single Accuracy Metric Collapses
The most useful part of RAG-X is not the headline gap; it is the vocabulary for classifying what happened underneath. The framework’s Context Utilization Efficiency, or CUE, divides outcomes into four quadrants: Effective Use, Information Blindness, Lucky Guess, and Correct Rejection.[1]
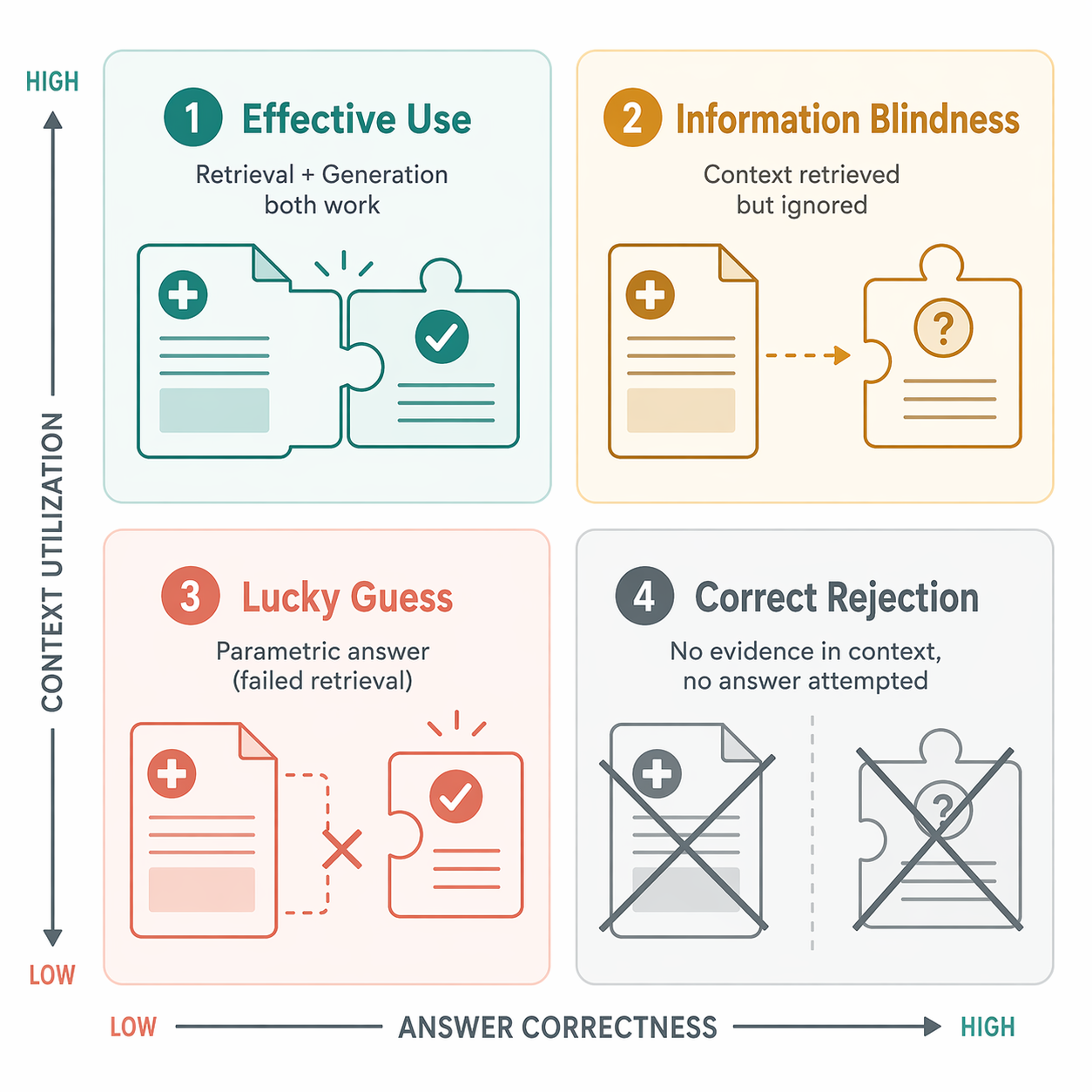
Effective Use is the case everyone wants: the retrieval step supplies useful evidence, and the model produces the correct answer using it. A validation report that can isolate this bucket is already more informative than one that simply announces accuracy. It tells reviewers that retrieval and generation worked together rather than merely coinciding.
Information Blindness is more operationally revealing. Here, relevant context is available, but the generator fails to use it correctly. That is not the same engineering problem as poor retrieval. The fix may involve prompt design, context ordering, answer constraints, model selection, or reasoning behavior under long context. Without this split, teams can spend weeks tuning retrieval when the failure is downstream.
Lucky Guess is the most dangerous bucket for accuracy-based validation because it is rewarded by the usual metric. The system gets the answer right even though the retrieved context did not support it. In the RAG-X MedQA pipeline, lucky guesses accounted for 33.9% of correct-looking answers.[1] That is not a harmless quirk. It means a visible portion of apparent success did not demonstrate the evidence behavior RAG is supposed to provide.
Correct Rejection is easy to undervalue in benchmark culture but essential in medicine. Sometimes the right behavior is to refuse, abstain, or indicate that the available evidence is inadequate. A system that can say “the retrieved material does not support a reliable answer” may be less dazzling than one that answers every question, but it is closer to the discipline clinical validation requires.
These categories do not solve medical RAG validation by themselves. They do something more modest and more necessary: they prevent different failure mechanisms from being averaged into one flattering number.
Retrieval Quality Is Not Just Recall
Once answer correctness and evidence use are separated, retrieval quality becomes harder to summarize with a single top-k score. RAG-X reported a 22% pairwise redundancy finding between top-ranked contexts.[1] In practical terms, a retriever may appear to return several pieces of evidence while actually returning overlapping fragments that do not broaden the evidentiary base.
Redundancy is not always bad. In some settings, corroborating evidence is useful. But in a constrained context window, redundant snippets can crowd out missing contraindications, exception criteria, or distinguishing clinical facts. If the generator later answers confidently, an evaluator needs to know whether the context set was genuinely informative or merely repetitive.
This is where medical RAG validation starts to diverge from generic search evaluation. It is not enough to ask whether any relevant document appeared near the top. Reviewers also need to know whether the retrieved material contained the decisive information, whether it conflicted with other retrieved material, whether it left the question underdetermined, and whether the generator behaved differently when the evidence was rearranged or degraded.
MedRGB Presses on Misinformation and Insufficient Evidence
MedRGB adds a complementary pressure test. Its value is not that it produces directly comparable numbers to RAG-X; it uses different test sets and evaluation protocols. Its value is that it asks whether models can handle corrupted or inadequate retrieved context rather than assuming retrieval is benign.
The benchmark reports that current LLMs may fail to detect factual misinformation in retrieved documents and may struggle in scenarios where the correct response depends on recognizing that the available evidence is insufficient.[2] That finding lands squarely on the clinical weakness of ordinary accuracy. If a system is tested mostly on questions where an answer exists and where the retrieved material is treated as trustworthy, the validation design may never observe the behavior needed when evidence is incomplete or misleading.
In medical work, insufficiency is not a corner case. A patient note may omit a relevant medication. A guideline excerpt may be outdated or too narrow. A retrieved abstract may discuss a population that does not match the patient. A knowledge base may contain a partial answer but not enough to justify a recommendation. A system that answers anyway can look fluent while transferring risk to the clinician who must detect the gap.
The operational implication is straightforward: validation sets need cases where the expected behavior is not answer production. They need insufficient-information items, contradictory-context items, and misinformation-resistance tests. Otherwise, a medical RAG system can be optimized for decisiveness rather than evidentiary discipline.
MIRAGE Shows Why Accuracy Gains Still Need Stress Testing
MIRAGE complicates the picture in a useful way. It reports that MedRAG can improve accuracy by up to 18% over chain-of-thought approaches, which is exactly the kind of result that makes RAG worth taking seriously in biomedical question answering.[3] Better retrieval can help. The point is not to dismiss RAG; the point is to validate the mechanism that produces the improvement.
The same benchmark also surfaces deployment-relevant effects, including lost-in-the-middle behavior and log-linear scaling problems.[3] Those are not cosmetic details. If evidence position changes model behavior, then a system may be sensitive to how retrieved passages are ordered inside the prompt. If scaling creates predictable but incomplete gains, then larger context or more retrieval may not remove the need for diagnostic evaluation.
This matters because an accuracy gain can be real and still be insufficient as a validation claim. A model can outperform a baseline while still mishandling evidence placement, redundant context, misleading snippets, or insufficient information. Clinical-grade validation has to preserve both truths: retrieval can improve medical QA performance, and the improvement can hide failure modes that ordinary answer scoring does not expose.
The Clinical Workflow Does Not See Benchmark Categories
Benchmarks are cleaner than clinical workflows. They usually isolate a question, define an expected answer, and score a response. Clinical work is messier: documentation is incomplete, relevant evidence is scattered, the user may be interrupted, and responsibility does not disappear because an AI system supplied citations.
A 2026 Nature discussion of RAG in clinical practice emphasizes caution around real-world deployment, including the need to consider clinical integration rather than treating technical retrieval performance as sufficient on its own.[4] That caution should not swallow the benchmark discussion, but it should set the standard. A validation result is only useful if it helps teams anticipate what will happen when the system is used in the presence of missing context, user trust, time pressure, and accountability.
There is also a boundary condition worth keeping visible: much of this evidence focuses on benchmarked question-answering behavior, often in relatively controlled or single-turn settings. It does not fully settle how a medical RAG system behaves across a longer clinical conversation, when earlier statements, corrections, and user assumptions can shape later answers. That is not a reason to ignore the benchmarks. It is a reason not to overclaim them.
What Validation Has to Add Before the Score Is Credible
A credible medical RAG evaluation should still report answer accuracy. Clinicians and developers need to know whether the system answers benchmark questions correctly. The mistake is treating that number as the validation endpoint rather than the beginning of the audit.
The minimum package is broader. It should include grounding-aware diagnostics such as Context Utilization Efficiency, so evaluators can distinguish effective use from information blindness, lucky guesses, and correct rejection. It should include sufficiency testing, so the system is rewarded for recognizing when retrieved evidence cannot support an answer. It should include robustness testing against misleading, contradictory, stale, or reordered context. It should include faithfulness checks that compare the generated answer with the retrieved material. And it should include context relevance checks, because irrelevant evidence can make an answer look documented without making it justified.
Tooling is beginning to make some of this easier, though tools do not remove the need for careful study design. NVIDIA’s evaluation guidance with Ragas describes LLM-as-a-judge methods for assessing faithfulness and context relevance in RAG pipelines.[5] Evidently AI similarly describes approaches for RAG evaluation, synthetic data generation, LLM-as-a-judge scoring, and production monitoring.[6] These are practical components, not clinical validation standards by themselves.
A validation plan for a medical RAG system should therefore ask questions that ordinary accuracy cannot answer:
- When the answer is correct, did the retrieved evidence actually support it?
- When the retrieved evidence is relevant, does the generator use it or ignore it?
- When the retrieved evidence is insufficient, does the system abstain, hedge appropriately, or fabricate certainty?
- When retrieved material contains misinformation or conflict, does the system detect the problem or amplify it?
- When context order, redundancy, or length changes, does the answer remain stable for the right reasons?
These questions also matter for governance. Broader discussions of generative AI evidence and policy in healthcare keep returning to the same practical issue: a system that performs well in a demonstration can still fail under the conditions that determine clinical trust. The same pattern appears in other generative AI tools, including ambient AI scribes, where surface fluency and task completion do not eliminate the need to inspect accuracy failures.
The Stricter Standard
RAG-X should not become a shrine. Its reported accuracy-grounding gap and lucky-guess rate are anchored to a specific experimental setup, and generalization across architectures, models, retrieval corpora, and clinical domains remains an empirical question. MedRGB and MIRAGE add pressure from different directions, but they do not produce one unified medical RAG validation standard.
Still, the direction is clear enough. Medical RAG system validation cannot stop at final-answer accuracy. The evaluation has to show whether the answer was supported, whether the retrieved evidence was relevant and sufficient, whether the generator used that evidence, and whether apparent success came from a lucky guess. A system has not been clinically validated merely because it answers benchmark questions correctly. It has been validated only when evaluators can identify when it is grounded, when retrieval has failed, and when the system only looks right.
References
- RAG-X: A Diagnostic Framework for Evaluating Retrieval-Augmented Generation in Medical Question Answering. arXiv. March 2026.
- MedRGB: A Benchmark for Medical Retrieval-Augmented Generation. arXiv.
- MIRAGE: Benchmarking Multi-hop Medical Reasoning with Retrieval-Augmented Generation. arXiv.
- Retrieval-augmented generation in clinical practice. Nature. 2026.
- Evaluating Medical RAG with Ragas. NVIDIA Developer Blog. 2026.
- RAG Evaluation: A Complete Guide to Evaluating Retrieval-Augmented Generation Systems. Evidently AI.
Comments
Join the discussion with an anonymous comment.