 Multiple (Johns Hopkins, Stanford, MIT Sloan, Harvard Medical School, Harvard Chan)
Multiple (Johns Hopkins, Stanford, MIT Sloan, Harvard Medical School, Harvard Chan)The Evidence for an AI Literacy Crisis in Healthcare
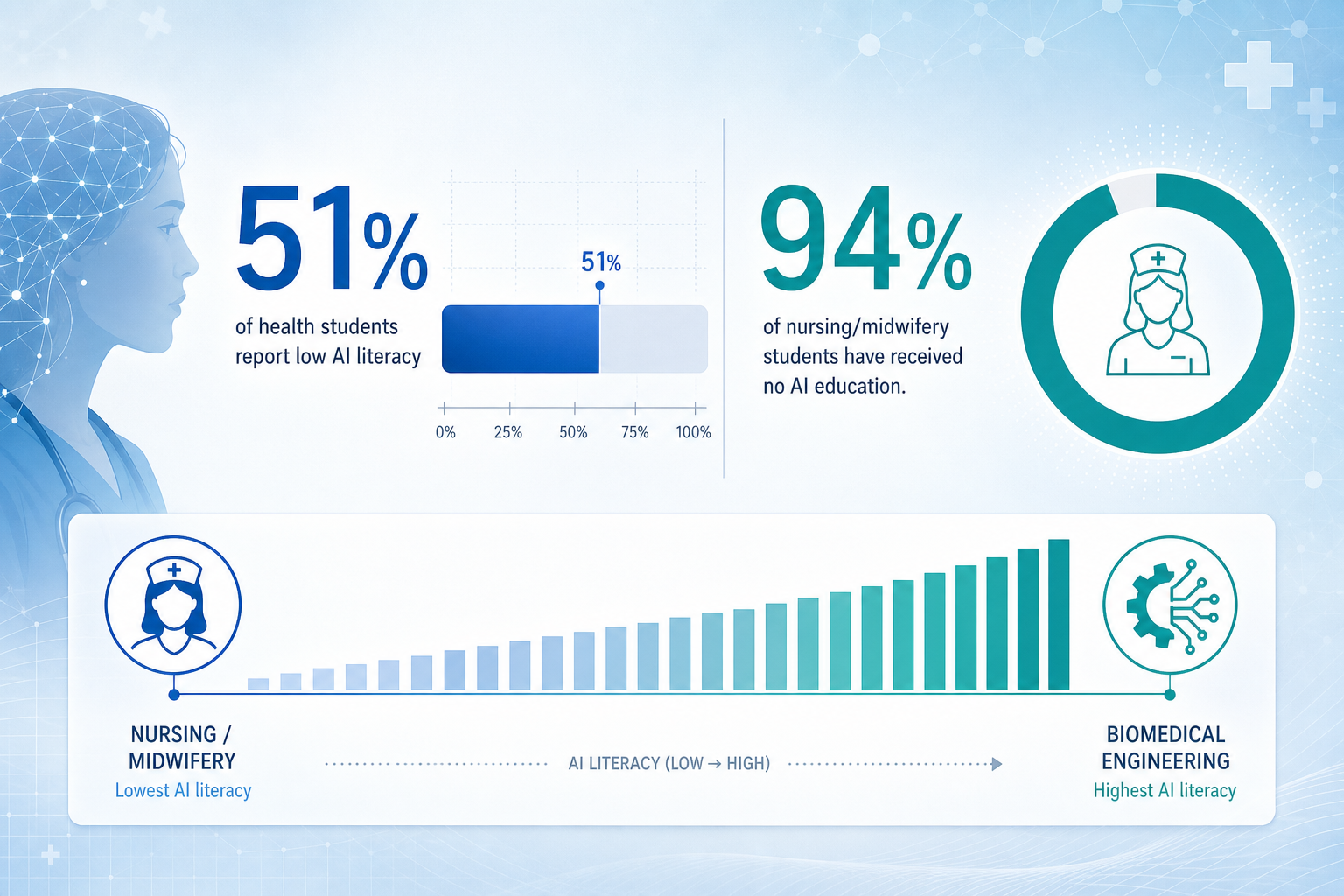
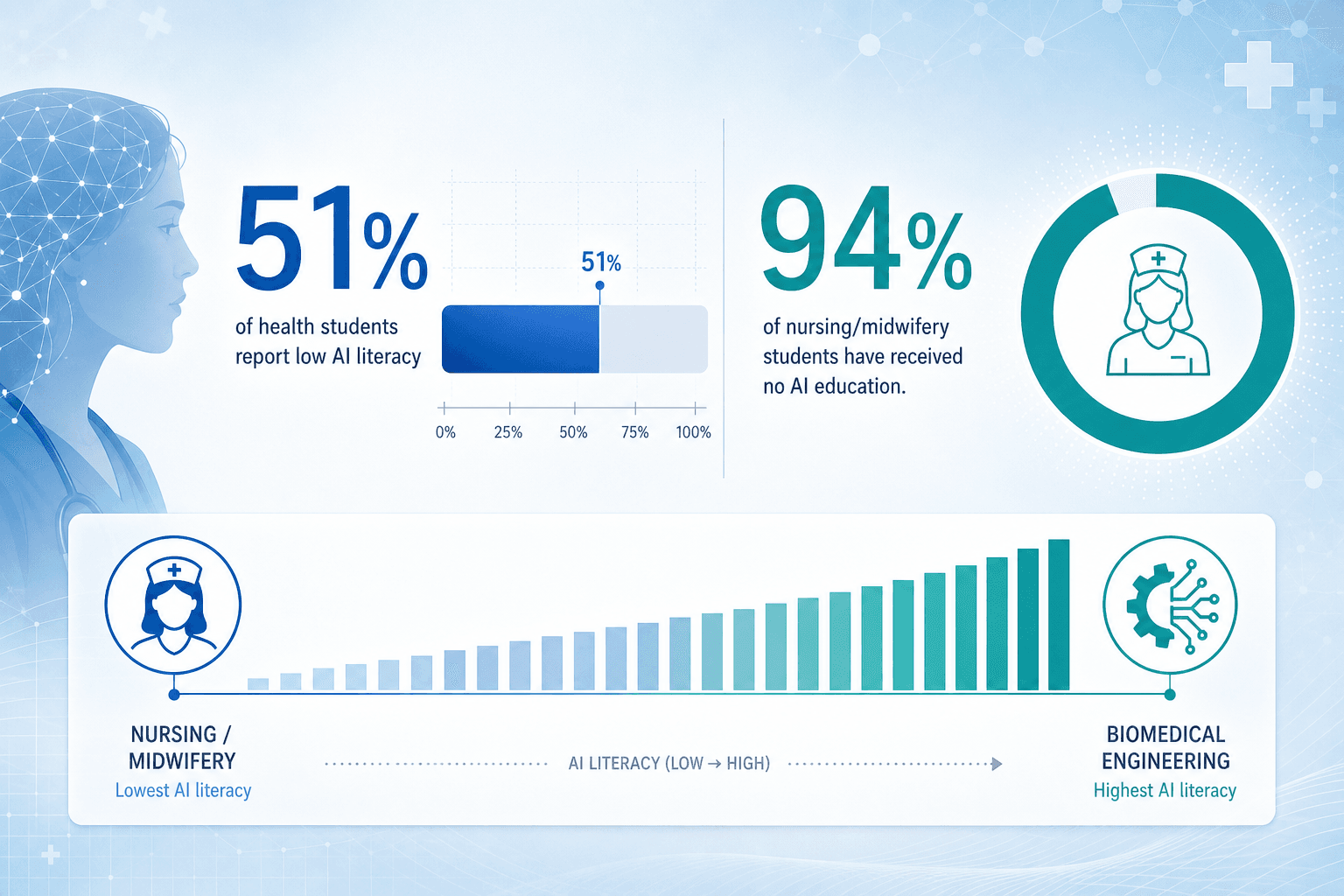
The gap between the pace of AI deployment in clinical settings and the workforce's readiness to use these tools is not a future risk — it is a present, measurable reality. A 2025 systematic review by Shishehgar et al. published in the International Nursing Review (PMC12183008) synthesized data from 12 studies encompassing 4,666 participants and found that 51% of health students self-reported low AI literacy. This figure is drawn from the largest single study in the review, a 2022 Canadian survey by Teng et al. of 2,167 entry-to-practice medical, nursing, and allied health students, which reported that 1,107 of 2,167 respondents (51.08%) rated their own AI knowledge as low.
The problem is even more acute in specific disciplines. A 2024 study by Erciyas et al. in Turkiye (n=500) found that 94% of nursing and midwifery students reported receiving no AI education whatsoever in their programs. This is not an isolated finding. A 2020 survey of 144 radiologists and radiology residents in Croatia by Dumić-Čule et al. found that 89.6% (95% CI: 0.83–0.94) agreed that AI education should be part of medical school curricula, with support consistently high across all age groups, subspecialties, and institution types.
The systematic review also revealed a troubling pattern in attitudes. Students intending to pursue research careers were significantly more positive toward AI than those planning clinical practice (p<0.001, Teng et al. 2022). This divergence suggests that the students who will be on the front lines of patient care — the ones most likely to interact with AI tools daily — are also the ones least prepared and least optimistic about them. Six out of the 12 studies in the review found that students agreed universities are the best setting for AI education (p<0.001), indicating a clear expectation that formal training institutions should take responsibility for closing this gap.
Disciplinary Variation: Who Needs AI Training Most?
AI literacy is not uniformly distributed across healthcare disciplines, and understanding these variations is essential for designing targeted educational interventions. A 2024 study by Aydinlar et al. examined AI literacy scores across different health science programs and found significant disparities. Nursing students consistently scored the lowest on AI literacy assessments, while biomedical engineering and medical students scored the highest.
| Discipline | Relative AI Literacy Level | Implication for Training |
|---|---|---|
| Nursing | Lowest | Urgent need for foundational AI literacy integrated into nursing curricula; focus on practical clinical applications and ethical considerations. |
| Allied Health (e.g., physiotherapy, occupational therapy) | Low to Moderate | Need for discipline-specific case studies showing how AI affects diagnostic and therapeutic workflows. |
| Pharmacy | Moderate | 75.1% of pharmacy students agreed AI reduces errors in medical practice (Syed et al. 2023, n=157); training should focus on clinical decision support and medication management AI. |
| Medicine | Moderate to High | Medical students show higher baseline literacy but still report gaps in regulatory knowledge and bias awareness. |
| Biomedical Engineering | Highest | May need less foundational AI training; focus on clinical translation, regulatory pathways, and interdisciplinary collaboration. |
These disparities matter because they reflect not just differences in baseline knowledge, but differences in the types of AI tools each discipline will encounter. A nurse using an AI-powered sepsis prediction system needs a different kind of literacy — understanding when to trust the alert, how to override it, and what data feeds it — than a radiologist evaluating an AI triage tool for chest X-rays. One-size-fits-all AI courses risk being too technical for some audiences and too superficial for others.
What Healthcare Professionals Actually Need to Learn
The evidence suggests that the market for healthcare AI courses is misaligned with what professionals actually need. Many programs emphasize machine learning algorithms, Python programming, or model-building exercises — skills that are relevant for data scientists but not for the vast majority of clinicians, administrators, and allied health professionals who will be users, not builders, of AI tools.
The systematic review by Shishehgar et al. identified four major themes in student and academic perceptions of AI education: limited AI literacy, the tension between AI as replacement versus support, optimism versus cautiousness, and ethical concerns. These themes point to a set of core competencies that any healthcare AI curriculum should address, beyond basic technical literacy.
- Ethics and Algorithmic Bias: Understanding how biased training data leads to unequal performance across demographic groups is not optional. A 2023 Bain report, cited by a Roche article, found that 75% of health system executives recognize AI's potential but only 6% have established concrete AI strategies — a gap that is partly driven by uncertainty about ethical and regulatory risks.
- Data Governance and Privacy: Clinicians need to understand how patient data is used to train and validate models, what consent models apply, and how to evaluate data provenance. This is especially critical as foundation models trained on broad internet data are increasingly applied to clinical tasks.
- Regulatory Frameworks: Professionals need working knowledge of FDA clearance pathways (510(k), De Novo, PMA), the EU AI Act's implications for medical devices, and emerging frameworks like the NIST AI Risk Management Framework. A course that does not cover regulatory context is incomplete for any healthcare audience.
- Clinical Integration and Workflow: The hardest part of AI deployment is not the model — it is the integration into clinical workflows, EHR systems, and existing decision-making processes. Courses should address implementation challenges, alert fatigue, and the human factors that determine whether a tool is adopted or abandoned.
- Evaluation of AI Evidence: Clinicians are trained to evaluate clinical trial evidence. They need equivalent skills for evaluating AI studies: understanding AUC, sensitivity, specificity, external validation, and the difference between a retrospective study and a prospective RCT.
Mapping Top-Tier Programs Against the Evidence-Based Needs
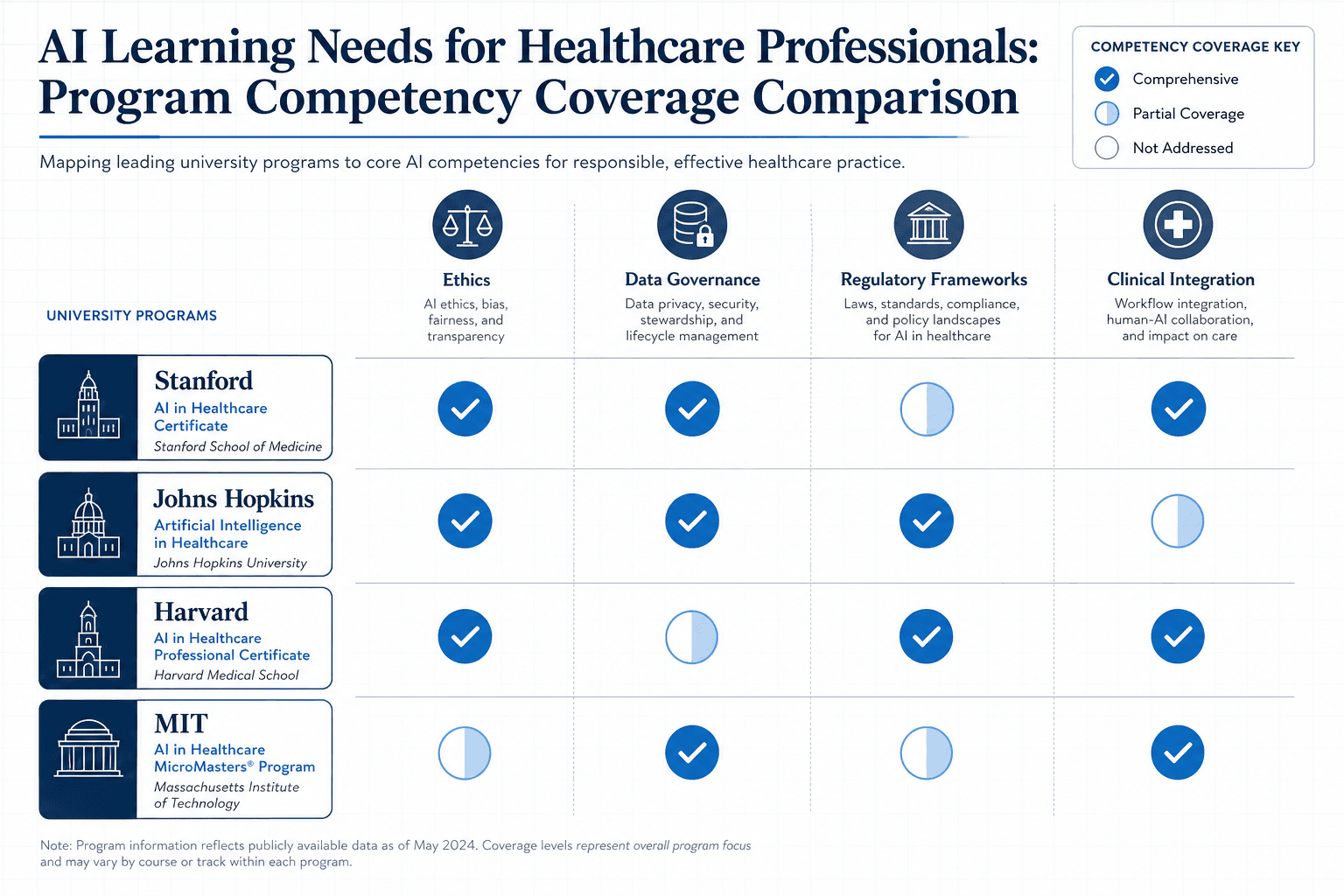
With the competency framework established, we can critically evaluate leading healthcare AI programs. The table below maps five prominent programs against the five core competency areas identified above. The goal is not to rank programs but to reveal where the market is meeting — and failing to meet — documented learner needs.
| Program | Format & Cost | Ethics & Bias | Data Governance | Regulatory Frameworks | Clinical Integration | CME / Accreditation |
|---|---|---|---|---|---|---|
| Johns Hopkins AI in Healthcare Certificate | 10 weeks, online, $2,990 | Covered (dedicated module on ethical AI) | Covered (data governance module) | Not explicitly covered in curriculum description | Covered (predictive analytics, LLMs in healthcare) | 6 CEUs from JHU |
| Stanford AI in Healthcare Specialization (Coursera) | 5 courses, self-paced, $79.99/month or free audit | Covered (module on AI impact on patient safety and quality) | Partial (data handling in capstone project) | Not explicitly covered | Covered (capstone on patient risk stratification) | CME accredited by Stanford Medicine |
| MIT Sloan Artificial Intelligence in Health Care | 6 weeks, self-paced online, $3,250 | Covered (interpretability and transparency modules) | Partial (data analytics module) | Not explicitly covered | Covered (disease diagnosis, patient risk stratification, hospital management) | 2.0 EEUs, MIT Sloan certificate |
| Harvard Medical School AI in Health Care: From Strategies to Implementation | 8 weeks, online, 4-6 hrs/week, cost ~$3,000-4,000 | Covered (bias and harm module, transparency/reproducibility) | Covered (AI development pipeline, data considerations) | Covered (regulatory landscape, FDA context) | Covered (real-world deployment challenges, case studies) | Certificate from Harvard Medical School |
| Harvard T.H. Chan School of Public Health AI in Health Care Certificates | 3-course or 5-course track, self-paced, ~$1,600/course | Covered (elective on innovation with AI) | Covered (business applications for AI course) | Partial (implementation course touches on regulatory issues) | Covered (implementing AI into clinical practice course) | Certificate of Specialization from Harvard Chan |
Several patterns emerge. First, regulatory frameworks are the most consistently under-addressed competency across all programs. Only the Harvard Medical School program explicitly covers FDA regulatory context in its curriculum description. Given that the FDA has now authorized over 1,000 AI/ML-enabled medical devices, and the EU AI Act is reshaping global market access, this is a significant gap.
Second, ethics and bias are now standard inclusions, which is a positive development. However, the depth varies considerably — from a single module in the JHU program to a dedicated module on bias and harm in the Harvard Medical School program. For clinicians who will be making real-time decisions with AI recommendations, superficial coverage of algorithmic bias is insufficient.
Third, clinical integration is well-covered across most programs, but the emphasis is often on technical integration (how to deploy a model) rather than human factors (how to train staff, manage alert fatigue, or handle false positives in a busy clinical workflow). The Harvard Medical School program's inclusion of real-world deployment challenges and case studies from organizations like Google Health and Sage Bionetworks suggests a more grounded approach.
The Curriculum Development Challenge: Integration Without Overload
The systematic review evidence is clear: students want AI education, and they believe universities should provide it. But there is a tension between this demand and the reality of already overcrowded health professional curricula. Medical students, nursing students, and allied health trainees are already struggling to absorb the core knowledge required for clinical practice. Adding a full AI course is not a trivial ask.
The review found that students intending research careers were more positive toward AI than those planning clinical practice (p<0.001). This may reflect a perception among clinically-oriented students that AI training is an additional burden rather than an integral part of their future practice. The challenge for curriculum designers is to demonstrate relevance — to show that AI literacy is not a separate subject but a competency that enhances diagnostic accuracy, reduces cognitive load, and improves patient outcomes.
Two models for integration are emerging. The first is the standalone course model, exemplified by the JHU, MIT Sloan, and Harvard Medical School programs. These are typically offered as continuing education or certificate programs for practicing professionals, not as part of core health professional curricula. The second model is embedding AI content across existing courses — for example, discussing AI-based diagnostic tools in a radiology rotation, or covering algorithmic bias in a medical ethics course. The systematic review found that six out of 12 studies supported the standalone model, with students agreeing that universities are the best setting for AI education (p<0.001).
For practicing professionals, CME-eligible programs offer a practical pathway. The Stanford/Coursera specialization is CME-accredited by Stanford Medicine, and the JHU program offers 6 CEUs. These programs allow clinicians to build AI literacy without returning to full-time study. However, the cost — $2,990 for JHU, $3,250 for MIT Sloan — may be a barrier for individual clinicians, particularly those in early career stages or in lower-resource settings.
Where the Market Is Falling Short
Despite the proliferation of healthcare AI courses, significant gaps remain between what the evidence shows professionals need and what the market delivers. These gaps are not trivial — they represent real risks for patient safety, regulatory compliance, and the effective deployment of AI tools.
- Regulatory Coverage Is Sparse: As noted in the program comparison, only one of the five major programs explicitly covers FDA regulatory frameworks. This is a critical omission. Clinicians and administrators who deploy AI tools without understanding their regulatory status — whether a device is 510(k)-cleared, De Novo authorized, or not cleared at all — are making decisions with incomplete information. For a deeper dive into the current regulatory landscape, see Artificial Intelligence and Health: The U.S. Regulatory Framework in 2026.
- Role-Specific Tracks Are Rare: Most programs target a generic 'healthcare professional' audience. Yet the AI literacy needs of a hospital CEO evaluating vendor contracts are fundamentally different from those of a radiologist using a triage tool or a nurse managing an AI-driven sepsis alert system. Programs that offer role-specific tracks — or at minimum, role-specific case studies — are the exception, not the rule.
- Outcome Evaluation Is Absent: None of the programs reviewed provide published evidence that completing their course actually improves clinical decision-making, reduces diagnostic errors, or changes deployment outcomes. This is a striking gap in a field that demands evidence-based practice. Healthcare professionals evaluating AI courses should ask: 'What evidence exists that this program changes behavior or improves outcomes?'
- Cost Barriers for Individual Learners: With flagship programs ranging from $2,990 to $3,250, the cost of AI education is prohibitive for many clinicians, particularly those in training or in lower-resource settings. Free options exist — the Stanford/Coursera specialization offers a free audit, and the AAFP offers a free 3-part course on AI in family medicine — but these are less comprehensive and lack the depth needed for advanced competency.
- Implementation Science Is Underemphasized: The hardest problems in healthcare AI are not technical — they are about workflow integration, staff adoption, and organizational change. Yet few programs dedicate significant time to implementation science, change management, or the real-world challenges documented in clinical deployment reports. For a grounded look at what deployment actually entails, see AI and Healthcare: What Real Clinical Deployments Actually Look Like.
Recommendations for Educators and Institutions
The evidence points to a clear set of actions for medical educators, health system administrators, and policy-makers who are serious about closing the AI literacy gap. These recommendations are grounded in the systematic review findings, the documented gaps in current course offerings, and the real-world challenges of AI deployment.
- Prioritize Ethics and Regulation in Every Curriculum: These are the most consistently under-addressed competencies across all major programs. Every healthcare AI course — whether for students or practicing professionals — should include dedicated modules on algorithmic bias, data governance, and regulatory frameworks. The NIST AI Risk Management Framework in Healthcare provides a useful structure for organizing this content.
- Develop Role-Specific Tracks: A single AI literacy course cannot serve clinicians, executives, IT professionals, and researchers equally well. Institutions should develop or adopt programs that offer differentiated content for each audience. For example, a track for nursing professionals might focus on AI-driven clinical decision support and alert management, while a track for executives would emphasize strategy, procurement, and regulatory risk.
- Leverage CME for Practicing Professionals: For the millions of healthcare professionals already in practice, CME-eligible programs are the most practical pathway to AI literacy. Institutions should subsidize access to accredited programs and provide protected time for completion. The Stanford/Coursera specialization (CME-accredited) and the JHU certificate (6 CEUs) are strong options for clinicians.
- Evaluate Programs Against Documented Learner Needs: Before selecting or developing an AI course, map its curriculum against the five competency areas identified in this article: ethics and bias, data governance, regulatory frameworks, clinical integration, and evidence evaluation. If a program covers only technical ML content without addressing these areas, it is incomplete for a healthcare audience.
- Invest in Implementation Science Training: The gap between AI tool approval and successful clinical deployment is wide, and it is primarily a human and organizational challenge, not a technical one. Courses should include content on change management, workflow redesign, and the evaluation of real-world deployment outcomes. For a comprehensive overview of current clinical applications and their evidence bases, see AI in Healthcare: A Structured Brief on Clinical Applications, Evidence, and Deployment Realities.
- Build Outcome Measurement Into Programs: The absence of published outcome data for AI education programs is a significant weakness. Institutions should design programs with built-in evaluation — measuring not just knowledge gains but also changes in clinical decision-making, tool adoption rates, and patient outcomes. This is the only way to move from 'we offered a course' to 'the course made a difference.'
The AI literacy gap in healthcare is not a theoretical concern — it is a documented, measurable problem with specific statistics, known disciplinary variations, and clear implications for patient safety and clinical effectiveness. The courses that will close this gap are not necessarily the most expensive or the most technically advanced. They are the ones that align their curricula with what the evidence shows professionals actually need: not just to understand AI, but to evaluate it, govern it, and integrate it safely into patient care.
Comments
Join the discussion with an anonymous comment.