 Multiple institutions (Harvard, ACPM, AAFP, Medmastery, MIT, University of Illinois, University of Florida)
Multiple institutions (Harvard, ACPM, AAFP, Medmastery, MIT, University of Illinois, University of Florida)The Confidence-Competence Gap: Why Enthusiasm Without Training Is a Patient Safety Problem
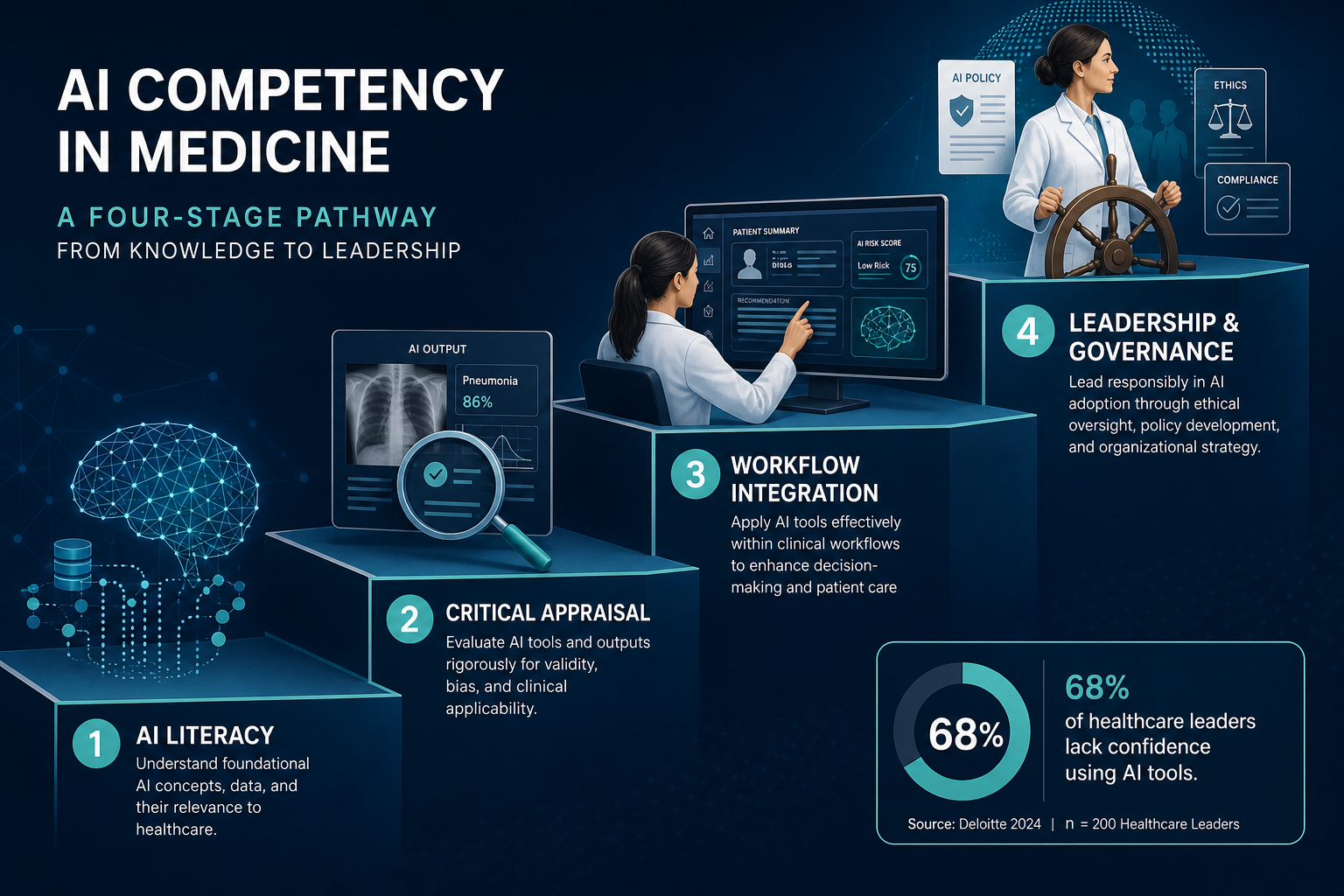
Healthcare professionals are not skeptical about artificial intelligence. A 2026 survey of 2,041 healthcare leaders across 90 countries, conducted by the Digital Medicine Society (DiMe) and Google for Health, found that the vast majority recognize AI's potential. Yet the same survey revealed a troubling disconnect: 68% of respondents did not feel "very confident" using or evaluating AI tools. Among clinicians specifically, 30% reported not using AI at all.
This is not a story about resistance to change. It is a story about a systemic training failure. The same survey found that 86% of clinicians rated insufficient training as a moderately or very difficult barrier to AI adoption. Enthusiasm is high; competence is not. And when clinicians lack the skills to critically evaluate AI outputs, understand model limitations, or detect when a tool is operating outside its intended use, the gap between hype and ability becomes a direct patient safety risk.
The problem is compounded by the speed of deployment. AI tools are already embedded in clinical workflows — radiology triage systems, ambient scribes, sepsis prediction algorithms, and clinical decision support platforms. Many of these tools received FDA clearance or authorization, but clearance does not guarantee that the clinicians using them understand the model's training data, its known failure modes, or the populations on which it was validated. Without structured training, the burden of safe use falls on professionals who were never taught how to evaluate the technology.
The goal of this article is to provide a clear, staged pathway from AI enthusiasm to genuine competency — grounded in published education models and mapped to real courses that exist today. The framework is designed for clinicians, researchers, and healthcare administrators who know they need to build AI skills but do not know where to start or what "competency" actually means in practice.
Why Competency Matters: Automation Bias, Governance Demands, and Real-World Deployment Realities
The case for structured AI competency goes beyond professional development. It is rooted in three concrete risks that emerge when AI tools are used by inadequately trained clinicians.
Automation Bias and the Erosion of Clinical Judgment
Automation bias — the tendency to over-rely on automated recommendations — is well documented in aviation and has been increasingly observed in clinical settings. When a clinician trusts an AI-generated diagnosis or treatment suggestion without critically evaluating it, errors that the model would have made go uncorrected. The Perspectives on Medical Education (PME) Journal, in a 2025 article proposing four core AI competencies for all physicians, specifically identified "effective AI partnerships" as a required skill: knowing when to use AI and when to question its outputs, and actively preventing automation bias.
This is not a theoretical concern. Real-world deployment reports show that AI tools can produce confident but incorrect outputs, particularly when applied to patient populations that differ from their training data. Without training in model evaluation and bias detection, clinicians lack the framework to recognize when a tool is failing.
Regulatory and Governance Demands Are Rising
Healthcare organizations are increasingly being held accountable for the AI tools they deploy. The NIST AI Risk Management Framework (AI RMF) provides a structured approach to governing AI systems through its four core functions: GOVERN, MAP, MEASURE, and MANAGE. The FDA continues to refine its oversight of AI/ML-enabled software as a medical device (SaMD). The EU AI Act imposes new requirements on high-risk AI systems used in healthcare. These frameworks place obligations not just on developers but on deploying organizations and the clinicians who use the tools.
A clinician who understands these governance structures is better equipped to participate in institutional AI procurement decisions, contribute to policy development, and ensure that the tools used in their practice meet appropriate standards of safety and transparency.
Integration Is Already Hard — and Training Is the Missing Piece
The DiMe survey found that 91% of clinicians who use AI rated integration difficulty as moderately or very difficult. The top barriers to AI adoption were workflow integration (72%), unclear leadership direction (68%), and limited staff capacity and training (61%). These numbers make clear that training is not a secondary concern — it is a primary barrier to safe and effective AI deployment.
For a deeper look at how AI tools are actually being deployed in hospitals and clinics today — including the integration challenges and documented failure modes — see our analysis of real clinical deployments.
A Staged Competency Model for AI in Medicine
To move from enthusiasm to competence, clinicians need a structured development pathway — not a random collection of courses. The PME Journal's 2025 article on AI education pathways proposed four core competencies for all physicians: AI literacy, effective AI partnerships, responsible AI use, and adaptability and resilience without AI. Building on that framework, and on the DiMe curriculum roadmap that defines three tracks (Critical Appraiser, Workflow Architect, and Governance Leader), we present a four-stage competency model tailored to the needs of practicing healthcare professionals.
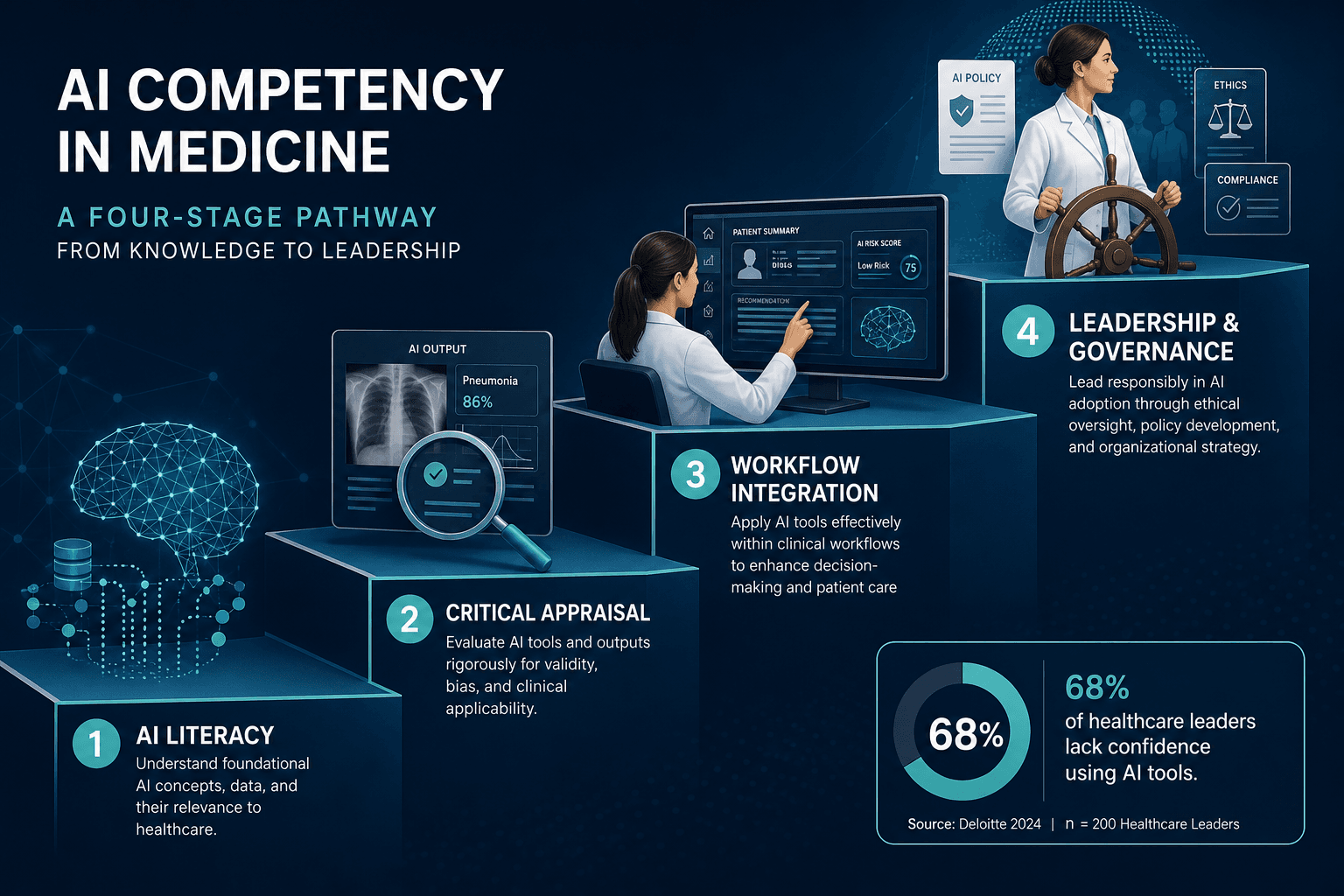
Each stage builds on the previous one. A clinician does not need to complete all four stages to benefit from training — but skipping stages creates gaps that can compromise safe use. The model is designed to be flexible: a medical student might start at Stage 1, while an experienced department chair might begin at Stage 2 or 3 depending on prior exposure.
- Stage 1: AI Literacy — Understanding what AI is, how models are trained, and what they can and cannot do.
- Stage 2: Critical Appraisal — Evaluating AI outputs, detecting bias, reading the evidence, and understanding regulatory status.
- Stage 3: Workflow Integration — Using AI tools safely in daily clinical practice, understanding EHR integration, and managing automation bias.
- Stage 4: Leadership and Governance — Shaping institutional AI policy, leading implementation, and ensuring accountability.
The sections that follow map each stage to specific courses and resources that are available as of mid-2026. These are not endorsements — they are structured directory entries designed to help you identify the right starting point based on your current knowledge and career goals.
Stage 1: AI Literacy — Understanding What AI Is and How Models Work
AI literacy is the foundation. Without a basic understanding of how machine learning models are trained, what terms like "supervised learning," "neural network," and "foundation model" mean, and why concepts like model drift and hallucination matter in clinical contexts, a clinician cannot meaningfully evaluate an AI tool's output.
The good news: Stage 1 is achievable in days, not months. Several high-quality, low-cost (or free) courses provide the conceptual foundation needed to move forward.
| Course | Format | Cost | Key Content | Target Audience |
|---|---|---|---|---|
| AAFP AI in Family Medicine: Transforming Your Practice | Self-paced, 3 parts | Free | AI basics, clinical use cases, practice integration overview | Clinicians (primary care focus) |
| Medmastery ChatGPT Essentials for Clinicians | Self-paced, 14 lessons | Free | Generative AI fundamentals, prompt engineering, clinical applications | All healthcare professionals |
| Massachusetts Medical Society AI Course | Self-paced | $40–$90 | AI terminology, clinical applications, ethical considerations | Physicians and medical students |
| ACPM AI in Preventive Medicine & Public Health Certification | Self-paced, 10 modules | Not disclosed | Fundamentals of AI/ML, algorithms, neural networks, supervised learning | Physicians and public health professionals |
The ACPM certification is particularly noteworthy because it is taught by physician subject matter experts in informatics, data science, and public health, and it offers 11.5 CME credits. Its first module covers exactly the foundational concepts — algorithms, neural networks, supervised learning — that define Stage 1 competency.
Stage 2: Critical Appraisal — Evaluating AI Outputs, Detecting Bias, and Reading the Evidence
Stage 2 moves from understanding what AI is to evaluating whether a specific AI tool is safe, effective, and appropriate for a given clinical context. This requires skills that most clinicians were never taught in medical school: interpreting study designs (RCT, prospective validation, retrospective cohort), understanding performance metrics (sensitivity, specificity, AUROC), detecting algorithmic bias, and assessing regulatory status (FDA 510(k), De Novo, PMA).
The PME Journal framework calls this "responsible AI use" — considering ethics, equity, and the environmental footprint of AI systems. It also overlaps with the DiMe "Critical Appraiser" track, which focuses on AI vigilance and safety for all clinicians.
| Course | Format | Cost | Key Content | CME |
|---|---|---|---|---|
| Harvard HMX: AI in Medicine — Foundations and Applications | Self-paced online | $495 | Supervised learning, generative modeling, pre-market evaluation, post-market surveillance, regulatory frameworks | Yes (AMA PRA Category 1) |
| ACPM AI Certification (Modules 2–5) | Self-paced | Included in certification | Ethical considerations, bias, health equity, regulatory/legal (HIPAA, FDA), clinical integration | 11.5 CME (full course) |
| University of Illinois AI in Medicine Certificate | Self-paced | $750 | AI in clinical practice, evidence evaluation, implementation strategies | Yes |
The Harvard HMX course is particularly strong on the regulatory side, covering both pre-market evaluation and post-market surveillance strategies for AI models, as well as different regulatory frameworks for AI in medicine. This is essential knowledge for any clinician who will be involved in selecting or overseeing AI tools.
For readers who want to go deeper on bias detection specifically, our glossary entry on algorithmic bias covers audit frameworks and mitigation methods in detail.
Stage 3: Workflow Integration — Using AI Safely in Daily Clinical Practice
Stage 3 is where theory meets practice. A clinician may understand how a model works and how to evaluate its evidence, but using it safely in a real clinical workflow — with all the interruptions, time pressures, and information overload that entails — requires additional skills.
The DiMe survey found that 91% of clinicians who use AI rated integration difficulty as moderately or very difficult. The top barrier to adoption was workflow integration (72%). This stage addresses those challenges directly: understanding how AI tools integrate with EHR systems (Epic, Oracle Health, Meditech), how ambient scribes capture and structure clinical notes, how clinical decision support tools present recommendations, and how to manage the cognitive load of interacting with AI during patient encounters.
| Course | Format | Cost | Key Content | CME |
|---|---|---|---|---|
| Harvard Medical School: AI in Clinical Medicine | Live online (June 11–15, 2026) | $2,500 | AI fundamentals, chatbots, ambient scribes, drug development, precision medicine, ethics, law, regulation, clinical implementation, specialty applications | Up to 27.50 AMA PRA Category 1 Credits |
| MIT: Solutions for the Future of Healthcare with AI | In-person / online | $2,600 | AI applications in clinical settings, implementation strategies, systems thinking | Yes |
| University of Florida AI-Based Medicine Technical Expertise CME | Self-paced | $200 | Python programming for AI, model deployment, clinical integration | Yes |
Harvard Medical School's AI in Clinical Medicine course, taught by faculty including Isaac Kohane, Arjun Manrai, and Adam Rodman, is the most comprehensive Stage 3 offering available. Its curriculum covers specialty-specific applications, ambient scribes, and clinical implementation — exactly the topics that bridge the gap between knowing about AI and using it safely.
Stage 4: Leadership and Governance — Shaping Policy, Leading Implementation, and Ensuring Accountability
The final stage is for clinicians who are moving into — or already occupy — leadership roles. These are the professionals who will shape institutional AI strategy, lead procurement decisions, develop governance frameworks, and ensure that AI deployment is aligned with patient safety and health equity goals.
The DiMe survey identified "unclear leadership direction" as the second most common barrier to AI adoption (68%). Stage 4 training addresses this gap by equipping leaders with the knowledge they need to provide clear, evidence-based direction.
| Course | Format | Cost | Key Content | Target Audience |
|---|---|---|---|---|
| Harvard: Leading AI Innovation in Health Care | Executive program | Not disclosed | AI strategy, governance, regulatory frameworks, organizational change management | Executives, department chairs, CMIOs |
| Harvard: AI for Health Care — Concepts and Applications | Self-paced / cohort | $2,600 | AI applications, implementation strategy, policy considerations | Clinical leaders and administrators |
| ACPM AI Certification (Modules 6–10) | Self-paced | Included in certification | Regulatory/legal, clinical integration, collaboration, public health AI strategy | Physicians and public health leaders |
Leaders at this stage should also be familiar with the NIST AI Risk Management Framework, which provides a structured approach to governing AI systems. Our analysis of the NIST AI RMF in healthcare explains how the GOVERN, MAP, MEASURE, and MANAGE functions apply to clinical AI deployment and how they bridge FDA voluntary governance and algorithmic accountability.
Your 30-60-90 Day Learning Plan: From Hype to Competency
The following plan is designed for a clinician or healthcare professional starting from minimal AI knowledge. Adjust the timeline based on your prior experience and available time.
| Timeframe | Stage | Recommended Actions | Estimated Time |
|---|---|---|---|
| Days 1–30 | Stage 1: AI Literacy | Complete AAFP free course (3 parts) or Medmastery ChatGPT Essentials (14 lessons). Learn key terminology: supervised learning, neural network, model drift, hallucination, AUROC. | 4–8 hours total |
| Days 31–60 | Stage 2: Critical Appraisal | Enroll in Harvard HMX AI in Medicine ($495) or ACPM AI Certification (Modules 1–5). Practice evaluating one AI study using the CONSORT-AI checklist. Learn FDA clearance pathways (510(k), De Novo, PMA). | 15–25 hours total |
| Days 61–90 | Stage 3: Workflow Integration | Identify one AI tool used in your specialty or institution. Observe its deployment, review its FDA clearance status and published evidence, and discuss its limitations with a colleague. Consider enrolling in Harvard AI in Clinical Medicine ($2,500, June 2026) or a specialty-specific course. | 10–20 hours (plus course time) |
Stage 4 (Leadership and Governance) is not included in the 90-day plan because it typically requires the foundation of the first three stages and is most relevant for professionals who have already taken on — or are preparing for — leadership roles. If you are in that position, consider adding a Stage 4 course to your 6- to 12-month development plan.
- First 30 days: Focus on free or low-cost resources. The goal is not mastery — it is vocabulary and conceptual orientation. You should be able to explain what a foundation model is, why model drift matters, and what AUROC measures.
- Next 30 days: Invest in a structured program that includes regulatory content and bias detection. The Harvard HMX course ($495) is the strongest option for self-paced learners. The ACPM certification is a good alternative if you prefer a physician-taught curriculum with CME credits.
- Final 30 days: Move from learning to doing. Identify a real AI tool in your clinical environment, review its FDA clearance and published evidence, and discuss its strengths and limitations with a colleague. If possible, observe a deployment in action.
Competency in AI is not a destination — it is a continuous process of learning, unlearning, and adapting as the technology evolves. The 68% of healthcare leaders who lack confidence in using AI tools are not failing individually; they are the product of a system that has not yet integrated AI training into professional development pathways. The goal of this staged framework is to provide a clear path forward — one that starts with basic literacy, builds critical evaluation skills, extends to safe clinical use, and ultimately prepares leaders to govern AI responsibly.
For readers who want to compare courses by role, background, and career goals rather than by competency stage, our structured decision framework for choosing an AI in healthcare course provides a complementary perspective.
Comments
Join the discussion with an anonymous comment.