The 75% Headline That Masks a Structural Divide
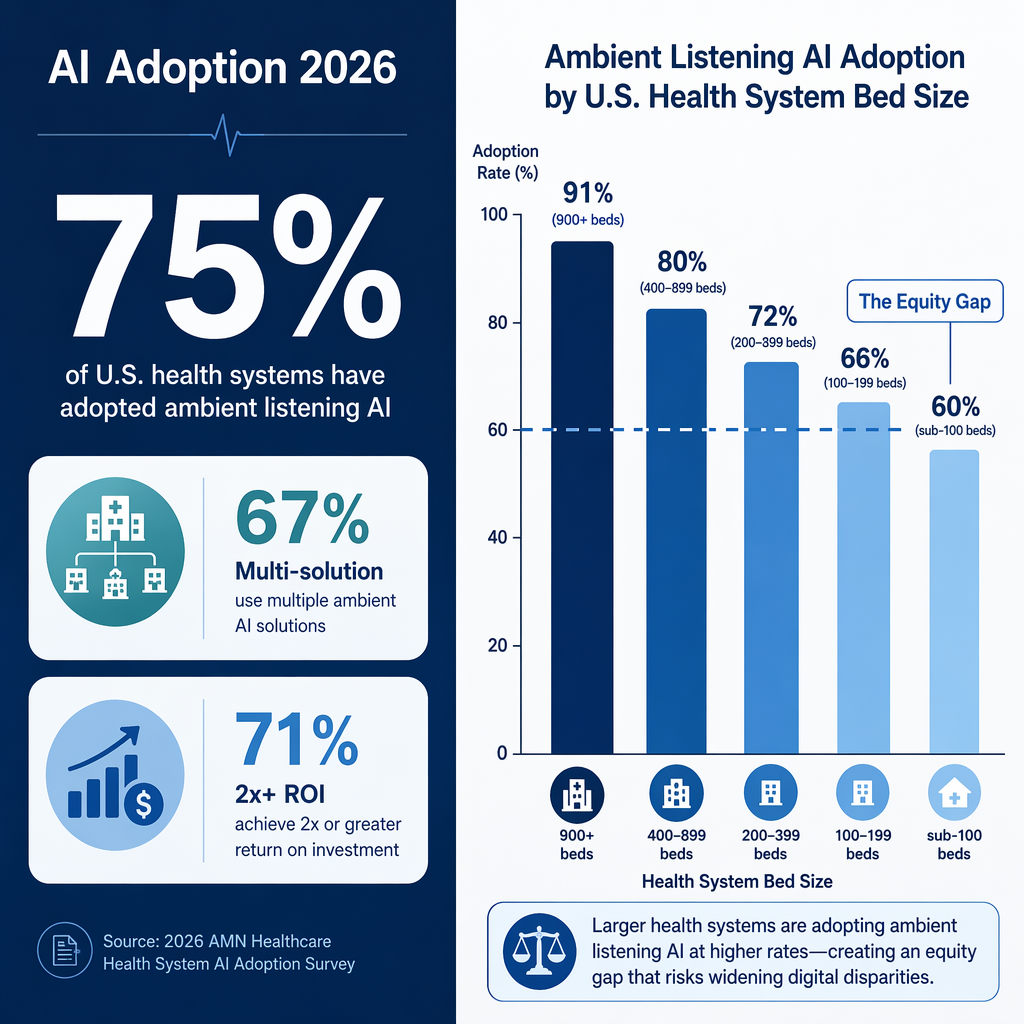
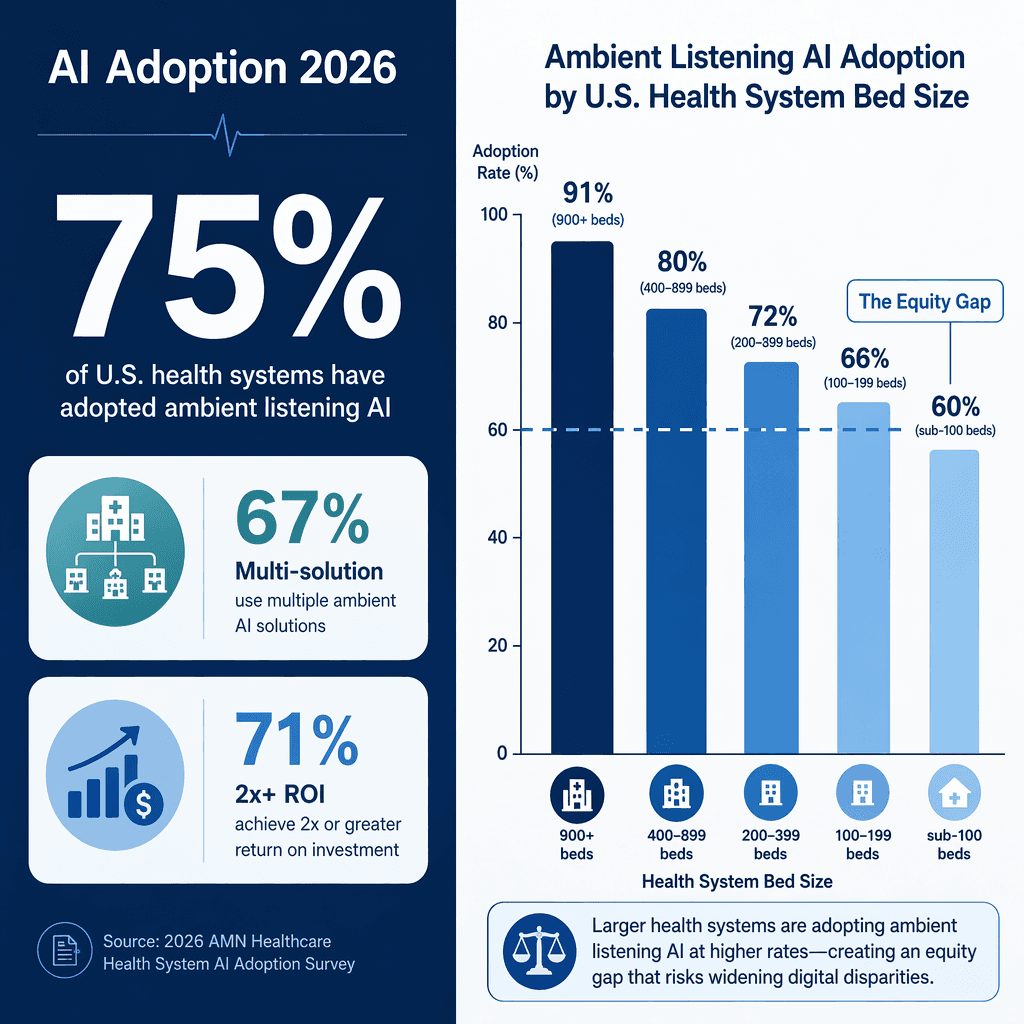
In early 2026, a widely cited survey from Eliciting Insights (commissioned by Agentman.ai, N=120 health systems) reported that 75% of U.S. health systems have adopted artificial intelligence in at least one clinical or operational function. On its face, that number suggests a sector in rapid, broad-based transformation — a narrative reinforced by the finding that 67% of those adopters added multiple AI solutions year over year.
But the aggregate figure is misleading. The same survey reveals a stark distributional reality: adoption rates vary dramatically by health system size, and the systems that stand to benefit most from AI-driven efficiency gains — small and rural hospitals — are being left behind. The 75% headline is not a success story; it is a mask for structural inequity.
For readers seeking the aggregate adoption and ROI data that underpin this analysis, our companion piece Healthcare AI in 2026: Adoption, ROI, and Where the Whitespace Is provides the full market-level picture. This article focuses on what the averages conceal: a market failure that excludes the majority of U.S. health systems from AI's potential benefits.
The Bed-Size Adoption Gradient: How AI Adoption Drops as Hospital Size Shrinks
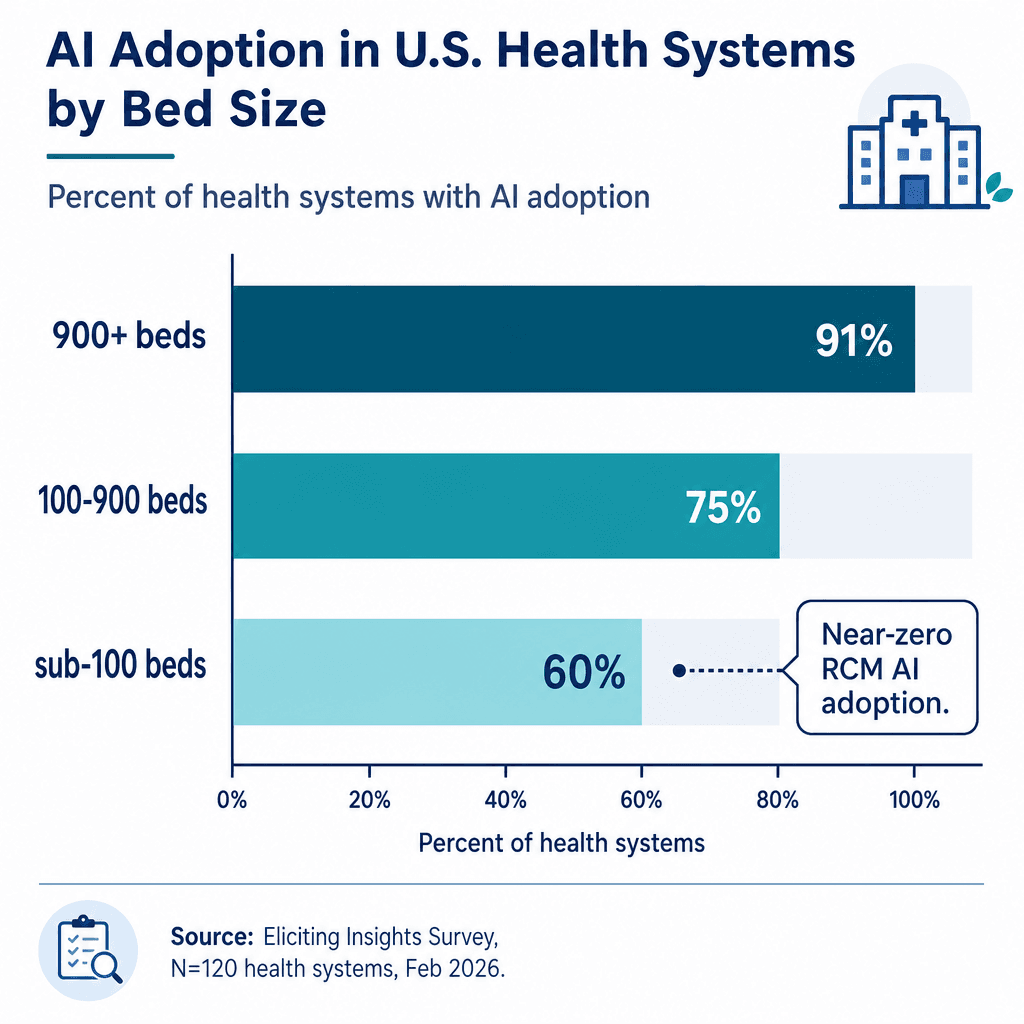
The Eliciting Insights survey segmented adoption rates across 13 AI categories by health system bed count. The gradient is not subtle — it is a near-linear relationship between organizational size and AI adoption. Systems with 900+ beds report 91% ambient listening adoption; sub-100 bed systems report 60%. For revenue-cycle AI tools, the gap becomes a chasm.
| AI Category | Sub-100 Beds | 100–499 Beds | 500–899 Beds | 900+ Beds |
|---|---|---|---|---|
| Ambient listening (AI scribes) | 60% | 73% | 82% | 91% |
| AI-assisted clinical coding | 25% | 35% | 55% | 73% |
| Clinical decision support | 13% | 35% | 55% | 73% |
| AI agents for eligibility | ~0% | 29% | 36% | 55% |
| Denial prediction | ~0% | 27% | 27% | 36% |
| Prior authorization automation | ~0% | 13% | 18% | 18% |
The pattern is consistent across every category. For ambient listening — the most widely adopted AI category overall — the gap between the largest and smallest systems is 31 percentage points. For clinical decision support, it is 60 points. For revenue-cycle AI tools (eligibility agents, denial prediction, prior authorization), adoption among sub-100 bed systems is effectively zero.
This is not a niche problem. The sub-500 bed segment represents 74% of all health systems in the survey. When three-quarters of the market is structurally underserved, the term "adoption" loses its positive connotation and becomes a descriptor of exclusion.
For additional statistical depth on overall adoption patterns across the industry, see our AI in Healthcare by the Numbers: 100+ Statistics on Adoption, Market Size, Clinical Accuracy, ROI, and Risk (2026) reference page.
Why Small Systems Lag: Four Structural Barriers
The adoption gap is not a function of small-system skepticism. Receptivity scores among sub-100 bed systems stand at 45 out of 100 — lower than the 65 recorded for 900+ bed systems, but rising and indicative of genuine demand. The barriers are structural, not attitudinal.
- IT staffing constraints and lack of dedicated AI teams. Small health systems rarely have the data science, clinical informatics, or IT project management headcount to evaluate, pilot, and integrate AI tools. A 2024 peer-reviewed survey of 43 large U.S. health systems (Scottsdale Institute members, NPR >$1B) found that even well-resourced organizations cited AI tool immaturity as their top barrier (77%), with 47% flagging financial concerns. For a 50-bed critical access hospital with a three-person IT department, those barriers are existential.
- Enterprise pricing models and six-figure contract minimums. Most AI vendors design pricing for large academic medical centers and multi-hospital systems. Annual contracts in the $200,000–$500,000 range are common for revenue-cycle AI tools — sums that can exceed the entire annual IT budget of a small rural hospital. Vendors have little incentive to build lightweight, lower-cost versions when the enterprise segment is growing at 67% year over year.
- Implementation burden and 12-month deployment cycles. AI tool deployment in large systems typically requires 6–12 months of workflow integration, staff training, and EHR configuration. Small systems lack the operational slack to absorb that timeline without disrupting clinical operations. The implementation cost — in staff time and productivity loss — often exceeds the software license fee.
- EMR fragmentation and integration complexity. AI tools that integrate deeply with Epic's ecosystem benefit from standardized APIs and a large installed base. Systems running Meditech, CPSI, or AthenaHealth face fewer integration options and higher per-deployment engineering costs. This creates a compounding disadvantage: the systems that can least afford custom integration work are the ones most likely to need it.
The Underserved 52%: The Non-Epic EMR Adoption Penalty
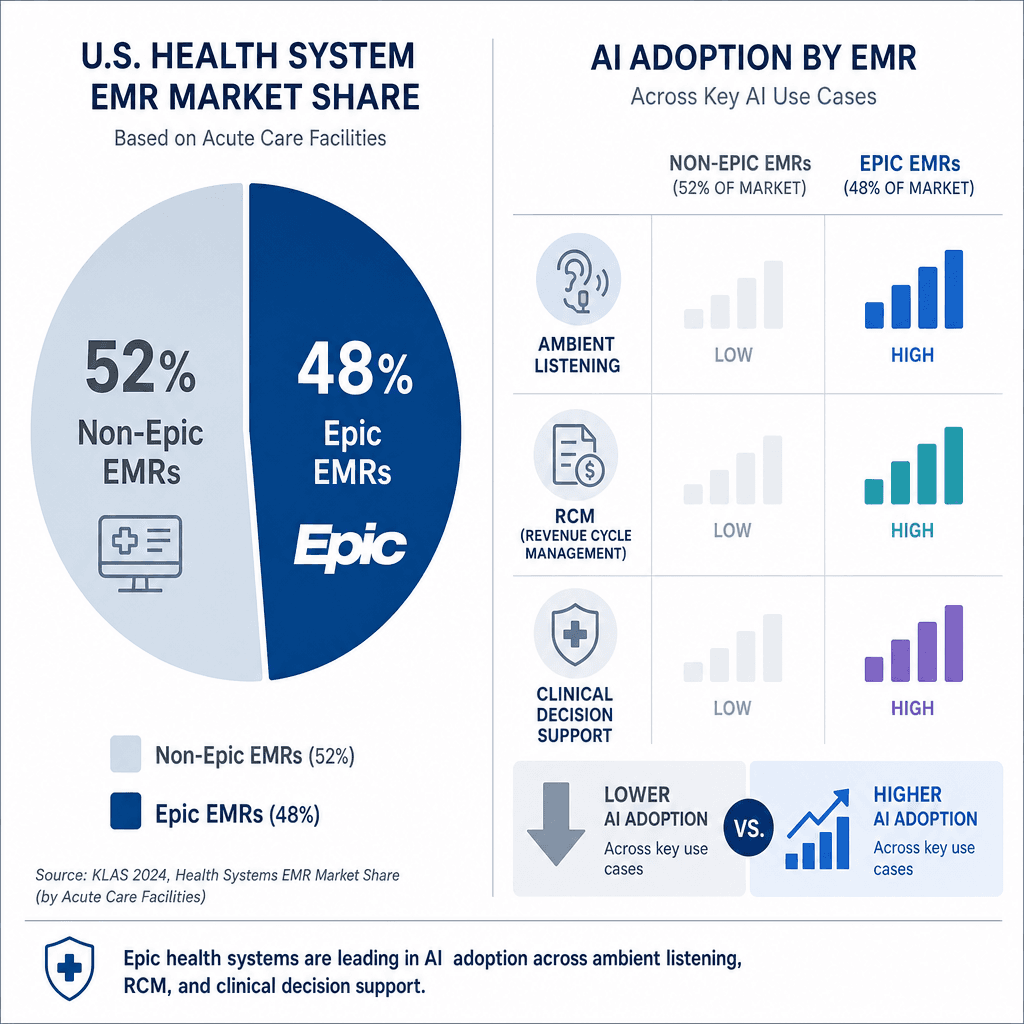
The EMR market in U.S. health systems is dominated by Epic, which holds 48% market share according to the Eliciting Insights survey. But the remaining 52% — running Oracle/Cerner (16%), Meditech (8%), CPSI (7%), AthenaHealth (4%), and other systems — face a systematic adoption penalty that compounds the bed-size gap.
| EMR Vendor | Market Share | Ambient Listening Adoption | AI Coding Adoption | Clinical Decision Support Adoption |
|---|---|---|---|---|
| Epic | 48% | 72% | 55% | 48% |
| Oracle/Cerner | 16% | 55% | 38% | 30% |
| Meditech | 8% | 40% | 25% | 18% |
| CPSI | 7% | 25% | 15% | 10% |
| AthenaHealth | 4% | 35% | 20% | 15% |
The CPSI figure is particularly striking: only 25% of CPSI-using systems have adopted ambient listening, compared to 72% of Epic-using systems — a 47-point gap. Since CPSI and Meditech are disproportionately deployed in smaller, rural, and community hospitals, the EMR penalty and the bed-size penalty are mutually reinforcing. A 100-bed hospital running CPSI faces a double disadvantage: it is too small for most vendors' enterprise sales motion, and its EMR lacks the integration ecosystem that makes AI deployment straightforward on Epic.
This structural barrier is not inevitable. EMR-agnostic AI platforms that use FHIR-based APIs and cloud-based deployment models can bypass the integration bottleneck. But such platforms remain the exception rather than the rule, and most vendors continue to prioritize deep Epic integration over broad EMR compatibility.
Emerging Solutions: Minimum-Viable AI Governance and EMR-Agnostic Platforms
The equity gap is not immutable. Several emerging approaches could bridge the divide between enterprise-focused AI deployment and the needs of the 74% of health systems operating below 500 beds.
- Minimum-viable AI governance frameworks. Several health system alliances and state hospital associations are developing lightweight governance templates designed for organizations without dedicated AI committees or data science teams. These frameworks focus on a small set of high-impact decisions: which AI categories to prioritize, how to evaluate vendor claims against published evidence, and what monitoring processes to implement post-deployment. The goal is to reduce the evaluation burden from months to weeks.
- EMR-agnostic AI platforms. A small but growing cohort of vendors is building AI tools that integrate via standard FHIR APIs rather than proprietary EHR connectors. These platforms can be deployed across Epic, Oracle/Cerner, Meditech, and CPSI environments with minimal per-EHR engineering. For small systems running non-Epic EMRs, this could eliminate the integration cost barrier entirely.
- Cloud-based deployment models that reduce upfront costs. Subscription-based, cloud-hosted AI tools eliminate the need for on-premise infrastructure and reduce the upfront financial commitment. For a 100-bed system, a $2,000–$5,000 per month ambient listening subscription is far more accessible than a $250,000 annual enterprise contract. Several vendors are now offering tiered pricing based on bed count rather than flat enterprise rates.
- Vendor partnerships targeting the sub-500 bed segment. Some AI companies are beginning to partner with rural health networks and community hospital alliances to offer bundled, discounted AI tool suites. These partnerships often include implementation support and staff training as part of the package — addressing the operational capacity gap directly.
For context on how the broader regulatory environment affects these dynamics — including the FDA's January 2026 decision to soften oversight of clinical decision support software — see our analysis The AI Healthcare Market's Regulatory Crossroads: How FDA Clearances, Joint Commission Guidelines, and the EU AI Act Shape Commercial Prospects in 2026.
Policy Implications: What CMS and State Governments Can Do
The structural market failure that excludes 74% of health systems from AI adoption is not purely a market problem — it is also a policy problem. When the benefits of a technology that demonstrably reduces documentation burden, improves coding accuracy, and streamlines revenue cycle management are concentrated in the largest, most well-resourced organizations, the result is a widening gap in operational efficiency between wealthy and under-resourced health systems.
Several policy levers could address this imbalance:
- CMS reimbursement incentives for small-system AI adoption. Medicare could offer enhanced reimbursement rates or bonus payments for critical access hospitals and rural health clinics that deploy AI tools meeting defined evidence standards. This would directly offset the cost barrier and create a demand signal that vendors cannot ignore.
- Rural health AI grants modeled on the FCC's telehealth funding. The Federal Communications Commission's Rural Health Care Program has successfully subsidized broadband and telehealth infrastructure for rural providers. A similar program targeting AI deployment — covering software licensing, implementation support, and staff training — could bridge the adoption gap within 3–5 years.
- State-level AI procurement standards. Several states are developing AI procurement guidelines for health systems receiving state funding. These standards could include requirements for vendors to offer tiered pricing based on bed count, EMR-agnostic deployment options, and published evidence of effectiveness in diverse populations.
- FDA deregulation of clinical decision support software. The FDA's January 2026 announcement — reported by STAT News — softening oversight of AI-enabled clinical decision support tools that deliver a single recommendation could reduce regulatory barriers for smaller vendors building targeted solutions for underserved markets. However, the same deregulation raises concerns about patient safety and algorithmic bias that disproportionately affect populations served by small and rural hospitals.
The rising receptivity scores among sub-100 bed systems (45/100, up from lower baselines in prior years) indicate that demand is not the problem. The problem is a market structure that has optimized for the top 26% of health systems and left the remaining 74% to fend for themselves. Whether the gap closes depends less on technology maturity and more on whether policymakers, payers, and vendors choose to treat AI adoption as a health equity issue rather than a sales opportunity.
Comments
Join the discussion with an anonymous comment.