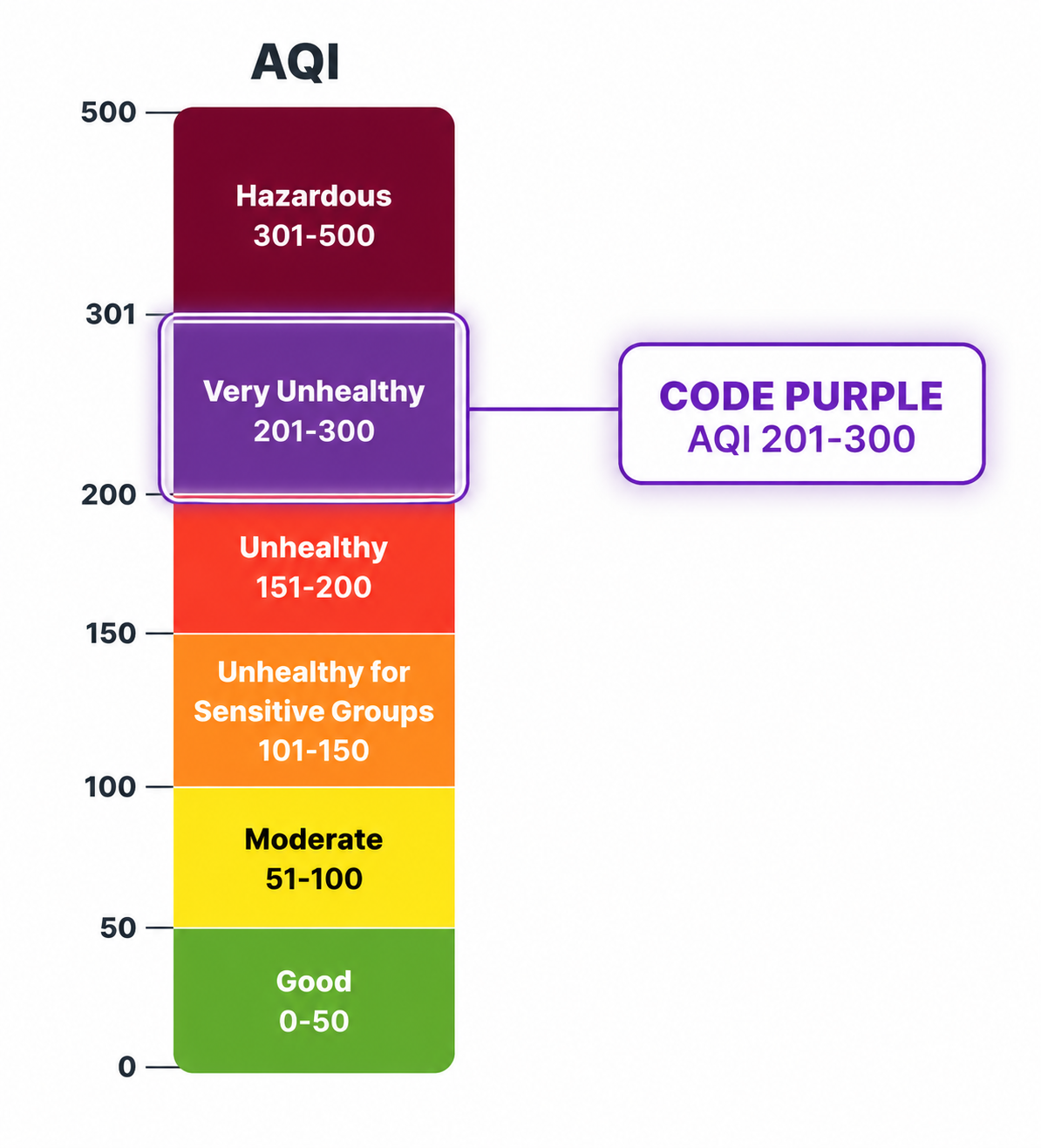
Code Purple air quality is the point on the Air Quality Index where the problem stops being framed only around sensitive groups. AQI 201–300 is “Very Unhealthy,” and EPA wildfire-smoke guidance treats that range as a level where public health officials should consider cancelling outdoor events such as concerts and competitive sports rather than asking people simply to tolerate the smoke better.[1]
That distinction matters during wildfire smoke events because the operational decision is rarely abstract. A school district has to decide whether recess, field trips, athletic practices, and summer camp activities move indoors. A parks department has to decide whether pools, fields, and outdoor programs stay open. A mayor’s office has to decide whether to distribute masks, open cleaner-air spaces, or activate shelter supports before respiratory harm shows up in emergency departments.
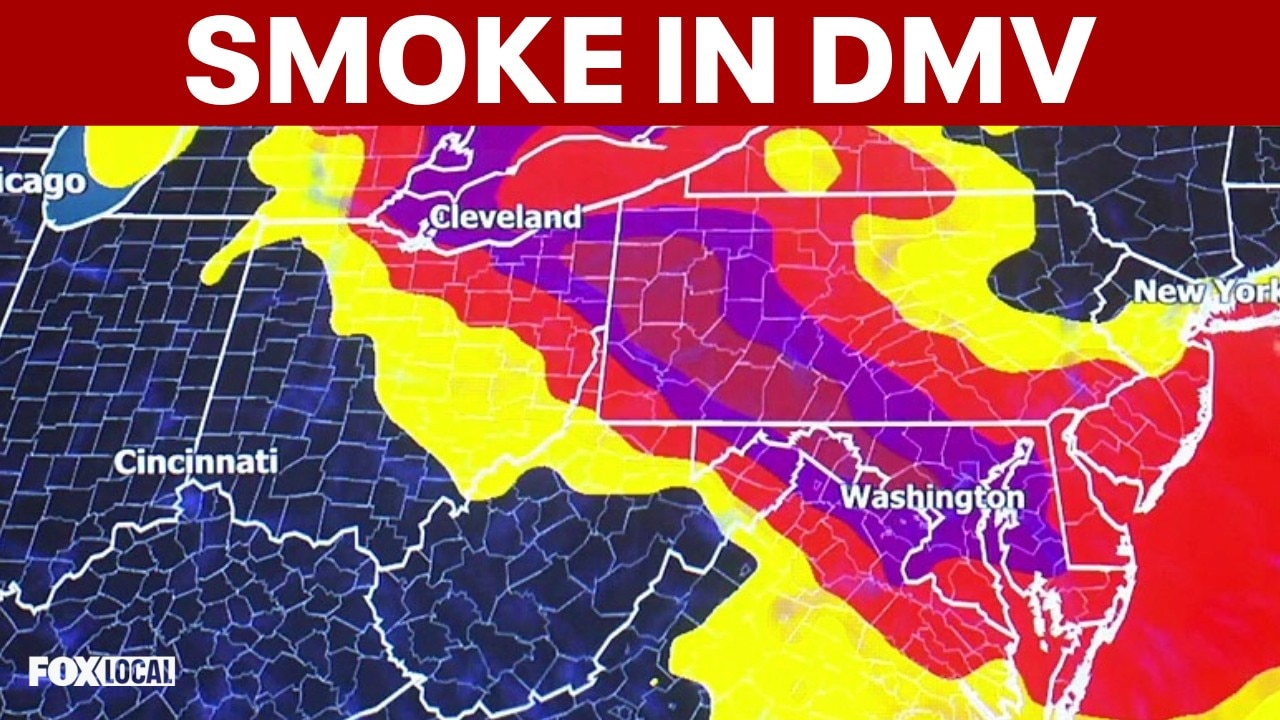
The July 2026 Canadian wildfire smoke event made those decisions visible across a broad stretch of the eastern and midwestern United States. Canadian fires sent smoke into multiple U.S. regions, with reporting describing hundreds of active fires and a season already ranking behind only 2023 in Canada’s recent fire record.[2] Forecast coverage described smoke affecting more than 100 million people across 18 states and Washington, DC.[3] In that setting, Code Purple was not a map color. It became a cancellation trigger.
Why Code Purple Is Treated as a Health Threshold
The strongest reason to take Code Purple seriously is not the color system itself. It is the body of evidence behind the pollutant driving most wildfire-smoke alerts: fine particulate matter, especially PM2.5 from wildfire sources.
A 2025 Nature Sustainability study by Zhang and colleagues examined wildfire-specific PM2.5 and respiratory hospitalizations across multiple countries and territories, using data through 2019. The study found that each 1 µg/m³ increase in wildfire-specific PM2.5 was associated with a 0.36% increase in all-cause respiratory hospitalizations, with a 95% confidence interval of 0.32% to 0.38%.[4]
That number can look small until it is placed in the right frame. It is not an estimate for one person standing outside once. It is a population-level association: when smoke exposure rises across a city, county, or region, the expected number of respiratory hospitalizations rises with it. During a widespread smoke episode, the affected population is large enough that small percentage increases become meaningful for hospitals, schools, long-term care facilities, and emergency managers.
The same study found an even stronger signal for influenza hospitalizations: a 0.79% increase per 1 µg/m³ increase in wildfire-specific PM2.5.[4] The study does not mean that wildfire smoke causes every respiratory hospitalization during a smoke event, and it does not prove the hospitalization pattern for July 2026 specifically. It does support a narrower but important conclusion: higher wildfire-specific PM2.5 exposure is associated with measurable increases in respiratory hospitalization risk.
The age pattern is also directly relevant to cancellations. Zhang and colleagues reported significantly higher risks for children 19 and younger and adults 60 and older compared with adults ages 20–59.[4] That is why school recess, youth sports, day camps, senior programs, and outdoor community events belong in the same operational conversation as formal medical alerts. The people most exposed are often not the people with the most power to leave.
The study also found that wildfire PM2.5 appeared more toxic per unit than non-wildfire PM2.5 across major respiratory disease categories.[4] That finding is important because a smoke-filled afternoon is sometimes treated as if it were merely a worse version of ordinary air pollution. The evidence suggests a more specific risk profile: the source of the particles matters, not only the concentration.
| Evidence Point | Decision-Relevant Meaning |
|---|---|
| 0.36% increase in all-cause respiratory hospitalizations per 1 µg/m³ wildfire-specific PM2.5 | Rising wildfire smoke exposure is associated with measurable respiratory burden at the population level. |
| 0.79% increase in influenza hospitalizations per 1 µg/m³ wildfire-specific PM2.5 | Respiratory infection-related admissions may be especially sensitive to smoke exposure. |
| Higher risks for children 19 and younger and adults 60 and older | Youth activities, elder programs, and public events need earlier protective decisions. |
| Wildfire PM2.5 more toxic per unit than non-wildfire PM2.5 | Officials should not treat wildfire smoke as interchangeable with ordinary bad-air days. |
| 25,321 annual respiratory hospitalizations attributed to wildfire-specific PM2.5 across eight studied countries | The burden is large enough to justify standing protocols rather than ad hoc judgment. |
| 42.4% of PM2.5-linked respiratory hospitalizations attributed to wildfire PM2.5 despite 17.1% of ambient PM2.5 | Wildfire smoke contributes disproportionate respiratory harm relative to its share of total PM2.5. |
The disproportionate burden is the finding that should change how officials read a smoke forecast. Zhang and colleagues estimated that wildfire PM2.5 contributed to 42.4% of PM2.5-linked respiratory hospitalizations while accounting for only 17.1% of ambient PM2.5.[4] If a pollutant source is responsible for a much larger share of health burden than its share of mass concentration, waiting for visible illness before acting is not a neutral choice.
How Guidance Turns Evidence Into Cancellations
Public health guidance exists because event organizers cannot run a hospitalization study every time smoke arrives. They need thresholds that are conservative enough to protect people and clear enough to defend when families, ticket holders, coaches, vendors, and staff object.
EPA’s wildfire-smoke guide gives that translation in plain operational terms: at AQI 201 or higher, public health officials should consider cancelling outdoor events, including concerts and competitive sports.[1] Washington State Department of Health guidance uses the same basic operational line for AQI 201 and above: cancel outdoor public events and activities. Oregon went further for youth in June 2026, updating its guidance to cancel all outdoor youth activities when AQI is greater than 150, a lower threshold that reflects children’s heightened vulnerability during smoke events.[5]
These thresholds do not claim that every person outdoors at AQI 201 will be hospitalized. They establish when the balance shifts for institutions responsible for groups. The organizer of a youth tournament, a public pool, or a city-sponsored concert is not making a private risk choice. The organizer is deciding whether to create a setting where hundreds or thousands of people inhale smoke while exercising, working, commuting, supervising children, or waiting in line.
That is also why cancellations can look abrupt from the outside. The public sees the announcement. The people responsible for the decision see the chain behind it: forecast, AQI category, expected duration, population affected, feasibility of moving indoors, staff exposure, communication time, transportation, and whether medically vulnerable participants have any practical way to opt out.
For organizations trying to act before the worst smoke arrives, forecast systems and venue-closure models can help with timing, but they do not replace the health threshold. ClinicalMind’s coverage of AI wildfire-smoke venue closure forecasting is useful here because the hard part is often not recognizing bad air after it arrives. The hard part is cancelling early enough for buses, staffing, permits, and public notices to change.
July 2026 Showed the Protocols in Motion
The July 2026 event should not be treated as proof that cancellations reduced hospitalizations; the reports available during the event are official releases and news accounts, not peer-reviewed outcome analyses. What the event does show is that multiple jurisdictions treated Code Purple and severe smoke as a basis for coordinated protective action.
Pennsylvania’s Department of Environmental Protection declared a Code Purple air quality alert for the entire state for Friday, July 17, as wildfire smoke spread across the region.[6] Washington, DC issued an elevated Code Purple alert and urged residents to follow health precautions.[7] Those are not symbolic notices. They are public triggers that let schools, agencies, employers, and event organizers point to a shared standard rather than arguing from personal comfort.
In Washington, DC, public schools cancelled outdoor activities including recess, physical education, athletic practices, and field trips during the Code Purple alert.[7] That kind of decision is often criticized as disruptive, and it is disruptive. But the alternative is to ask children to absorb a risk that the evidence and guidance already identify as elevated, often while running, playing, or waiting outside for transportation.
Richmond, Virginia reported a range of event changes on July 17, including outdoor cancellations and schedule adjustments as smoke affected the city.[8] Baltimore-area coverage described Code Purple conditions and local disruptions, including public-facing changes tied to unhealthy air.[9] Across affected cities, the pattern was not one isolated cancellation. It was a municipal operating posture: reduce outdoor exertion, move what can be moved, close what cannot be made safe, and communicate before people arrive.
- Sports and recreation: competitive sports and outdoor recreation schedules were postponed or changed when smoke reached dangerous levels.[1][3]
- Schools and youth programs: DC Public Schools cancelled outdoor activities during the Code Purple alert, and Oregon’s June 2026 youth guidance supports even earlier cancellation for children at AQI above 150.[5][7]
- Municipal services and public facilities: parks, pools, and outdoor city services were closed or adjusted in affected jurisdictions rather than treated as routine operations.[8][9]
- Protective supports: cities used measures such as mask distribution and shelter or hotline supports for residents who could not simply stay inside.[7][9]
The protective-support piece deserves more attention than it usually gets. Telling people to stay indoors assumes they have clean indoor air, stable housing, air conditioning, control over work conditions, and the ability to skip outdoor obligations. Many do not. At Code Purple, cancelling events is only one part of the public-health response; cleaner-air access, respiratory protection, and outreach to unhoused residents and outdoor workers matter because exposure is not evenly distributed.
The same logic applies inside health systems. Hospitals and clinics may need to reschedule procedures, adjust staffing, or anticipate respiratory demand during smoke events. ClinicalMind’s article on smoke forecasts and emergency surgery cancellations shows the parallel: once smoke risk becomes operational, the question shifts from whether the air looks bad to whether the institution can safely continue as planned.
The Limits of a Single AQI Color
AQI categories are useful because they are simple enough for public communication. They are also incomplete. A person sitting quietly outdoors for a short period does not receive the same dose as a soccer player sprinting for an hour, a lifeguard on a full shift, a road worker, or a child with asthma waiting outside after school. Exposure duration, exertion, indoor filtration, baseline health, and the ability to leave all change the real risk.
Guidance also varies by jurisdiction. Oregon’s youth threshold is lower than the EPA’s AQI 201 cancellation point for broader outdoor events.[1][5] That does not make one threshold fake and the other real. It reflects different target populations, legal responsibilities, and risk tolerance. A youth program may reasonably cancel at a level where an adult-only activity might first modify, shorten, or move indoors.
There is also a timing limitation in the evidence. Zhang and colleagues analyzed data through 2019, so the study cannot directly measure hospitalization outcomes from the July 2026 smoke event or account for every post-COVID change in respiratory vulnerability, care-seeking, or hospital capacity.[4] The July 2026 accounts show what agencies and cities did during the event; they do not yet show how many hospitalizations were prevented.
That distinction is important for decision-makers who need both humility and resolve. The evidence does not promise that cancellations eliminate harm. It supports the public-health rationale for reducing preventable exposure when wildfire PM2.5 reaches levels associated with broader respiratory risk.
What the Cancellation Decision Is Really Saying
At Code Purple, the cancellation decision is not a claim that every outdoor event would produce a medical emergency. It is a judgment that the institution should not create avoidable mass exposure when official guidance says the air is very unhealthy and epidemiological evidence links wildfire-specific PM2.5 to increased respiratory hospitalization risk.
That is a defensible standard. It gives school administrators cover to cancel recess before children are coughing in the nurse’s office. It gives parks officials a reason to close pools before lifeguards and families spend hours in smoke. It gives event organizers a basis for postponement before attendance, staffing, and travel lock people into exposure. It gives local governments a reason to pair cancellations with masks, cleaner-air access, and outreach to people who cannot protect themselves by choice alone.
Code Purple health risks and event cancellations belong in the same decision because the threshold is built for action. The evidence is not perfect, and the AQI color does not capture every exposure detail. But at AQI 201–300, cancelling outdoor events is not cautious optics. It is a population-health intervention supported by observed respiratory risk signals and by guidance designed for exactly this kind of wildfire-smoke event.
References
- EPA Wildfire Smoke Guide for Public Health Officials, EPA, link
- Canada fires US air quality, BBC, link
- Smoke forecast relief, CNN, link
- Respiratory risks from wildfire-specific PM2.5 across multiple countries and territories, Nature Sustainability, 2025, link
- OHA updates guidance for youth outdoor activities during wildfire smoke air pollution events, Oregon Health Authority, June 8, 2026, link
- DEP declares Code Purple air quality alert for all of Pa. on Friday as wildfire smoke spreads, WVIA, July 16, 2026, link
- Air Quality Alert in Washington, DC Elevated to Code Purple; Mayor Bowser Urges Residents to Follow Precautions, DC Mayor Bowser, link
- Richmond air quality event changes, WTVR, July 17, 2026, link
- Alert Day: Code Red unhealthy air quality in Maryland, WBAL-TV, link
Comments
Join the discussion with an anonymous comment.