The claim does not leave the building as “an AI output.” It leaves as the provider’s reimbursement request. If the code is unsupported, overbilled, inconsistent with payer edits, or impossible to reconstruct months later, the explanation that a model suggested it will not answer the audit letter.
That is the compliance starting point for AI in medical coding in 2026. The operational pressure is real: physician billing work has been associated with substantial administrative cost, and one JAMA study estimated that billing and insurance-related activities consumed significant physician and staff time across encounter types.[1] Coding-related denials and billing errors are not abstract workflow irritants; they become delayed cash, refund demands, payer scrutiny, and, in the wrong circumstances, false-claim exposure.

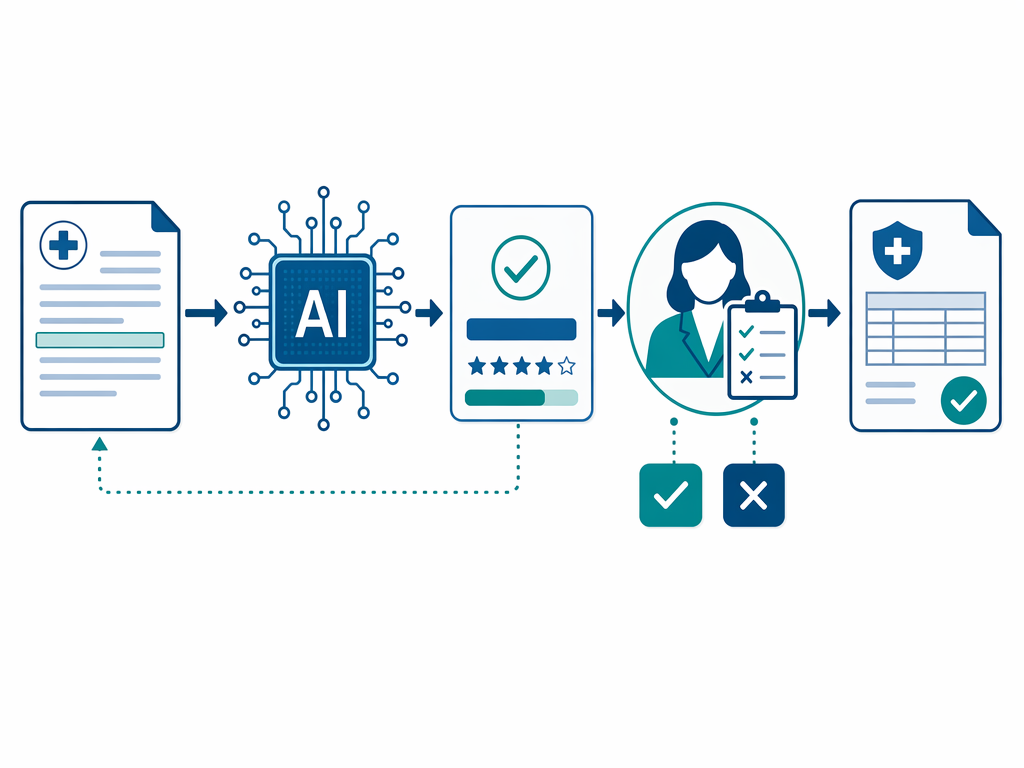
The useful question is no longer whether AI can accelerate coding. Many health systems are already evaluating it as part of broader AI revenue cycle management programs. The harder question is what the organization must be able to prove before the first AI-assisted code is submitted: who reviewed it, what documentation supported it, whether the system expressed uncertainty, whether a reviewer changed the recommendation, which edit logic applied, and how long that evidence remains retrievable.
Start With Classification, But Do Not Stop There
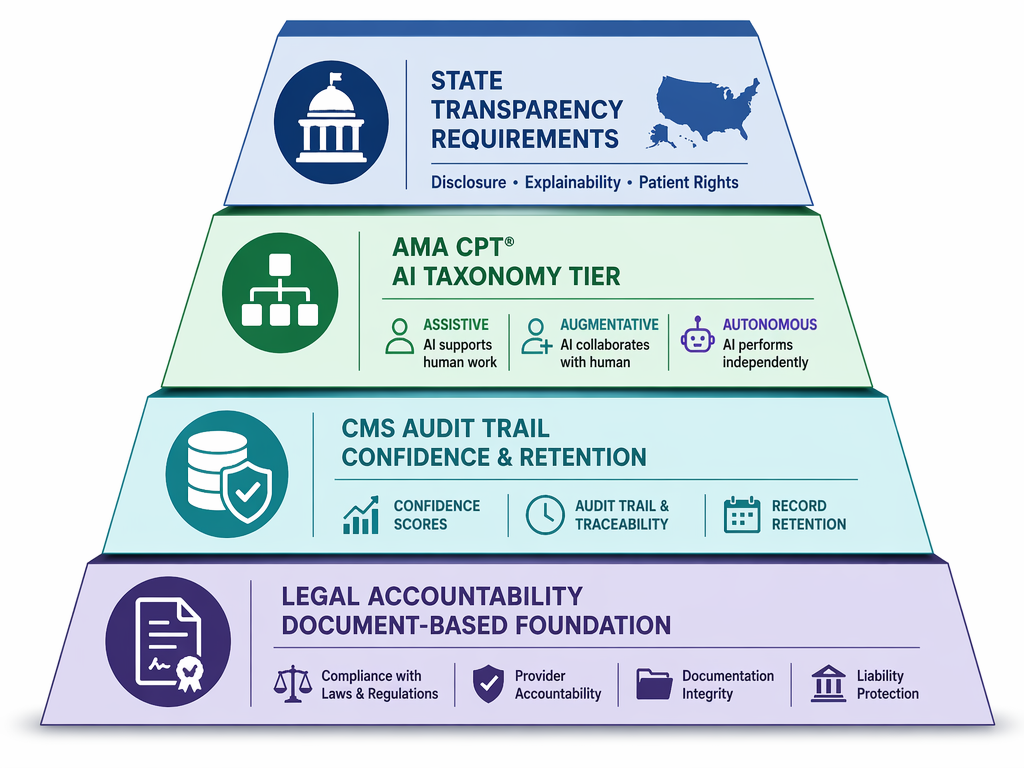
The AMA CPT AI taxonomy matters because it gives compliance teams a vocabulary for distinguishing tools that merely assist a person from tools that perform more independent clinical or administrative functions. A 2026 vendor compliance guide describes three tiers: Assistive, Augmentative, and Autonomous, with different billing and oversight implications depending on the level of human involvement.[2] The taxonomy details should be verified against primary AMA materials before a health system builds policy around them; the source cited here is secondary and vendor-published.
That caveat is not academic. If a procurement file says a product is “assistive,” but the implemented workflow allows the system to select codes, route clean claims, and bypass meaningful human review, the label will not carry the control environment. Compliance should classify the actual workflow, not the sales description.
| Question to Answer Before Go-Live | Why It Matters |
|---|---|
| Does the tool only suggest codes, or can it select and advance them? | This determines whether human review is a genuine control or a nominal step. |
| Is the reviewer required to see the supporting documentation sentence? | This connects the final code to the medical record rather than to a model-generated rationale. |
| Are confidence scores retained with the claim record? | This preserves evidence of system uncertainty at the time of coding. |
| Are overrides logged as structured data? | This lets the organization show when a human accepted, rejected, or changed the AI recommendation. |
| Can the system reproduce the coding path months or years later? | This is the practical difference between automation and audit readiness. |
Classification should therefore sit at the front of the governance file, but it should not be treated as the governance file. The tier tells the organization what kind of tool it thinks it has. The audit trail shows what actually happened to the claim.
The False Claims Act Problem Is Not AI-Specific, Which Is Exactly the Point
There is no need to invent a special “AI coding liability” doctrine to see the risk. The claim is submitted by or on behalf of the provider. The reimbursement flows to the provider or its billing entity. The documentation obligation belongs to the provider. A vendor contract may allocate service obligations or indemnity between private parties, but it does not turn an unsupported code into a supported one.
That is why AI coding compliance should be treated as an extension of established billing controls, not as a technology pilot that happens to touch claims. If an AI system assigns a higher-level evaluation and management code, adds a modifier, or selects a procedure code that is not supported by the record, the compliance question is the same one auditors already ask: what evidence supported the claim when it was submitted?
The answer cannot be “the model was accurate in aggregate.” Aggregate performance may matter during vendor selection, and ClinicalMind has separately covered the medical coding accuracy evidence. But aggregate accuracy does not defend an individual claim. A payer, contractor, or government investigator will care about the specific encounter, the specific documentation, the specific code, and the specific decision path.
This is where health systems can misread “human in the loop.” A coder who clicks accept on a queue of AI-suggested codes is not automatically a meaningful control. The organization needs to define what the reviewer is accountable for reviewing, what information is visible at the time of review, when escalation is required, and whether productivity targets create pressure to rubber-stamp the recommendation.
CMS-Ready Audit Trails Require Claim-Level Evidence, Not Dashboard Comfort
A governance program for AI-assisted coding should be designed around claim-level reconstruction. The 2026 guidance cited here describes the need to log AI confidence scores, human reviewer overrides, and final code selections at the claim level, with retention for at least seven years.[2] Whether a health system frames this as a CMS audit-trail requirement, a payer audit-readiness requirement, or an internal control standard, the operational consequence is the same: the evidence must be stored where compliance can retrieve it by claim, encounter, patient, date of service, code, reviewer, and version of the tool.
Procurement teams should translate that requirement into contract and architecture questions before implementation. A product demonstration that shows fast code suggestions is not enough. The health system needs to know whether the confidence score is exported, whether it is retained after final billing, whether reviewer changes overwrite the original AI recommendation, and whether the system preserves the documentation excerpt used to justify the code.
The highest-risk design is one that improves throughput while flattening the record. If the final claim shows only the submitted code, and the AI recommendation, confidence score, source sentence, and reviewer action live in a vendor interface that is not retained or not easily exportable, the compliance office will be reconstructing a decision without the decision record.
What the Audit Record Should Preserve
- The AI-suggested code or code set before human review.
- The confidence score or comparable uncertainty indicator available at the time of review.
- The exact documentation sentence, phrase, or structured field the system used as support.
- The human reviewer’s identity, role, action, and timestamp.
- Any override, rejection, downgrade, modifier change, or escalation.
- The final code submitted on the claim and the payer-specific edits applied before submission.
- The model, ruleset, or product version in use when the recommendation was generated.
This is not just an IT logging exercise. It changes how legal, compliance, revenue cycle, HIM, and procurement divide responsibility. Legal needs retention and access rights. Compliance needs monitoring reports that identify override patterns and high-risk code families. Revenue cycle needs workflows that do not bury uncertain recommendations inside productivity queues. IT needs integration that keeps the coding evidence tied to the claim record even if the vendor relationship ends.
Those requirements should appear in the statement of work. If the vendor cannot retain claim-level confidence and override data for the required period, the system may still be operationally attractive, but it is not ready for compliant deployment. If the vendor can retain the data only inside its own portal, the contract should address export, audit access, termination assistance, and data format.
Source Grounding Is the Bridge Between Automation and Defensibility
Source grounding is the practice of requiring the AI system to point back to the specific clinical documentation that supports each code. The 2026 vendor guide describes this as a compliance-oriented mitigation for hallucination risk: the system should highlight the sentence in the clinical record that justifies the code rather than merely produce the code and a narrative explanation.[2]
Grounding does not make a code correct. A sentence can be misread. A condition can be documented but not reportable. A procedure can be present in the note but bundled, excluded, or unsupported for the payer context. But grounding forces the review back to the record, which is where coding compliance lives.
A useful reviewer screen therefore should not show only “recommended code” and “accept.” It should show the documentation source, the model’s confidence, relevant coding guidance or edit warnings, and a structured way to accept, reject, or modify the recommendation. A free-text comment box is not enough if the organization later needs to analyze override rates, identify recurring model failures, or respond to payer questions.
For denial prevention, this matters because a clean-looking claim can still be fragile if the support is not retrievable. AI tools used for denial prevention in revenue cycle management should be evaluated not only on whether they reduce front-end defects, but also on whether they preserve the claim story for back-end review.
Payer Edits Still Control the Claim
AI coding systems do not displace payer-specific rules. National Correct Coding Initiative edits, local coverage rules, payer policies, modifier requirements, and plan-specific billing instructions still determine whether a code combination is payable and defensible. A model trained on documentation patterns can still generate a code combination that fails an edit or invites a denial.
The compliance control is not simply to run edits somewhere before submission. The organization should be able to show which edits were applied, when they were applied, and what happened when an AI recommendation conflicted with an edit. If the edit engine suppresses, changes, or flags a code, that action belongs in the same claim-level record as the AI recommendation and human reviewer action.
This is also where payer-provider automation dynamics become uncomfortable. Payers are expanding automated review and claims management capabilities while providers are automating coding and denial response. ClinicalMind has covered this broader AI arms race in revenue cycle management. For compliance purposes, the lesson is narrow: faster claim generation increases the need for stronger pre-submission controls, not weaker ones.
State Transparency Laws Add a Patchwork Layer
State AI transparency laws are developing unevenly, and multi-state health systems should assume that administrative AI use may trigger different disclosure, notice, governance, or documentation expectations depending on jurisdiction. The most visible activity has involved utilization management, prior authorization, and claims review, but coding cannot be isolated from that regulatory environment when it feeds claim submission and payment.
The practical problem is not that every state has the same rule. It is that the organization needs a deployment map. Which entities are using the tool? Which patient populations and payer lines are affected? Does the tool influence only internal coding, or does it affect patient-facing communications, coverage determinations, payment appeals, or administrative decisions that a state law treats differently?
For parallel context, ClinicalMind’s coverage of AI in prior authorization and claims-review regulation is the better place to track the broader state and federal transparency fight. In the coding context, the compliance takeaway is to avoid a single national rollout policy that ignores state-by-state disclosure and governance obligations.
Vendor Claims Need a Different Standard of Proof
Vendor materials can be useful, but they should be read as vendor materials. A narrative review on automated medical billing describes AI’s potential role in billing automation and revenue cycle improvement, while noting the context and limitations of the literature it reviews.[3] Vendor publications commonly emphasize accuracy, efficiency, workflow integration, and return on investment.[2][4] Those may be legitimate procurement considerations, but none of them substitute for the compliance record attached to a submitted claim.
The same caution applies to market-size estimates. Market research can show that AI coding is attracting investment and adoption attention, but it does not show that health systems have implemented the governance architecture needed to defend AI-assisted claims.[5] Adoption is not effectiveness, and effectiveness is not auditability.
This distinction matters for smaller and resource-constrained systems. A large academic health system may be able to build custom interfaces, retain structured logs, and run periodic coding audits. A smaller organization may receive the same product pitch without the same compliance infrastructure. ClinicalMind has described this implementation divide in health tech AI readiness, and it is directly relevant here: the legal obligation to defend a claim does not shrink because the IT team is small.
A Governance Framework Before the First AI-Assisted Claim
A defensible program should be in place before go-live, not assembled after the first payer dispute. The framework does not need to be ornate, but it does need named owners, written controls, retrievable evidence, and monitoring that can detect when the tool is creating risk rather than reducing work.
- Classification: document the tool’s AMA AI taxonomy category as implemented, and verify the category against primary AMA materials before relying on it.
- Accountability: define which role is responsible for final code review, when escalation is required, and how reviewer performance is monitored.
- Source grounding: require each AI-recommended code to link to supporting documentation visible to the reviewer.
- Audit trail: retain the AI recommendation, confidence score, reviewer action, override, final code, edit results, and tool version at the claim level.
- Retention: confirm that claim-level AI coding evidence remains accessible for the required retention period, including after vendor termination.
- Payer logic: map NCCI edits, payer-specific rules, modifier policies, and coverage requirements into the pre-submission workflow.
- State law mapping: identify where AI use in coding, billing, claims, or administrative decisions triggers disclosure or transparency obligations.
- Monitoring: review override rates, high-confidence errors, low-confidence acceptances, denial patterns, and coder productivity pressure.
The monitoring piece deserves particular attention. If the system’s high-confidence recommendations are often overridden in one specialty, that may signal a model problem. If reviewers almost never override low-confidence recommendations, that may signal a workflow or incentive problem. If denials cluster around a code family after implementation, compliance should not wait for an external audit to ask whether the model changed coding behavior.
Governance should also include periodic sampling by humans who are not simply the same coders clearing the queue. The sample should compare the final submitted code against the source documentation, the AI recommendation, the reviewer’s action, payer edit results, and any denial or payment outcome. That is how the organization learns whether the tool is improving coding integrity, merely increasing speed, or creating a new category of hard-to-see errors.
Broader CMS policy on automation and administrative decision-making is evolving beyond coding, including prior authorization and related oversight frameworks. For that wider regulatory context, see ClinicalMind’s analysis of CMS prior authorization and AI policy. For coding, the immediate control remains concrete: preserve the evidence that explains why this code was submitted for this encounter.
Compliance Readiness Is a Claim-Level Standard
A health system is not ready for AI-assisted coding merely because the vendor reports accuracy gains, offers a human-in-the-loop workflow, or integrates with the EHR. Those features may be helpful. They are not the same as a defensible claim.
Readiness means the organization has verified the applicable taxonomy, preserved claim-level evidence, defined reviewer accountability, retained confidence and override data, mapped payer and state disclosure duties, and made source-grounded coding reviewable under audit. Until those pieces are in place, the system may be automating coding work, but the provider is still carrying the liability without the record it will need when someone asks why the claim was billed that way.
References
- Administrative Costs Associated With Physician Billing — JAMA / PubMed, 2018.
- AI in Medical Coding 2026: Accuracy and Compliance — HelpSquad.
- The Evolution of Automated Medical Billing With AI — PMC / Cureus.
- AI Medical Coder: How It Works, Accuracy & ROI — RapidClaims.
- AI in Medical Coding Market Size — Towards Healthcare.
Comments
Join the discussion with an anonymous comment.