The practical difference in AI scribe vs medical transcription starts before a note exists. An AI scribe listens to a live patient-clinician encounter, runs the audio through speech recognition and language-model processing, and drafts a structured clinical note soon after the visit. Medical transcription usually begins after the clinician dictates or records a report; the service then converts that recording into text, often with human or AI-assisted review, and returns it later.[1][2]
That sounds like a speed comparison, but speed is the least interesting part. These are different documentation pipelines. They listen to different things, produce different artifacts, fail in different ways, and ask the signing clinician to review different kinds of risk.

| Comparison point | Ambient AI scribe | Medical transcription |
|---|---|---|
| Primary input | Live encounter audio between patient and clinician | Dictated or recorded clinician speech |
| Typical output | Structured note, often SOAP or DAP style; some products include code suggestions | Transcribed text from dictated clinical speech |
| Timing | Usually near real time or soon after encounter end | Commonly delayed, with 24-48 hour turnaround described in industry comparisons |
| Main review task | Check for omissions, hallucinated details, incorrect attribution, and note structure | Check word accuracy, terminology, formatting, and completeness of dictated content |
| Best fit | Conversational outpatient encounters where the clinical story unfolds in the room | Operative, procedural, radiology, pathology, and dictated reports |
Two Pipelines, Not One Pipeline at Different Speeds
An ambient AI scribe is built around the encounter. It captures conversation, identifies medically relevant content, filters out some irrelevant talk, and turns the visit into a note format the clinician can edit. Many tools aim for SOAP or DAP-style output, and some paid tiers add ICD-10 or CPT code suggestions to the draft.[1][2]
Traditional transcription is built around dictation. The clinician decides what to say into a recorder or microphone, often after the visit, procedure, imaging interpretation, or pathology review. The transcription process converts that dictated speech into text and returns it for review. The important distinction is that transcription does not need a natural conversation. It needs a clinician who can narrate the clinical facts clearly.
That difference matters most in the places where there is little or nothing useful for an ambient system to overhear. A primary care visit may contain the history, symptoms, counseling, plan, medication discussion, and patient questions in one continuous exchange. An operative report does not. A radiology report is not produced from a patient-clinician conversation at the bedside. A pathology report is not waiting inside ambient room audio. In those settings, dictation is not an old habit that forgot to die; it is the natural source document.
This is why a clinic can reasonably use AI scribes for exam-room documentation and still keep transcription for procedural or diagnostic reporting. The decision is not ideological. It follows the clinical source material.
What Each Model Produces
The output of an AI scribe is usually more interpretive than a transcript. It is not simply a cleaned-up record of every word spoken. The system selects details, places them into a clinical structure, and may phrase the plan in the style expected by the EHR note. That can be useful when the clinician wants to leave the visit with a draft note rather than a block of raw dialogue.
The same feature creates the first review obligation. The clinician is not just proofreading words. They are checking whether the note preserved the clinical meaning of the encounter: what was actually said, what was decided, what was deferred, what the patient declined, and what should not be in the chart at all.
A transcription output is usually closer to the dictated source. That does not make it automatically safer or easier. If the clinician dictated a vague assessment, the transcript will not repair the clinical reasoning. If the audio quality is poor or terminology is misheard, the text can still be wrong. But the review task is more tightly tied to the words the clinician intentionally supplied.
The workflow consequence is simple: AI scribes reduce the need to compose a note from scratch, while transcription reduces the need to type what has already been dictated. Those are different burdens.
Accuracy Is Not a Single Scoreboard
The least helpful comparison is the one that places an AI scribe hallucination rate next to a transcription word-error rate and declares a winner. A peer-reviewed commentary in npj Digital Medicine describes AI scribe hallucination rates around 1-3%, while speech-recognition transcription error rates for medical jargon have been reported around 7-11%.[3] Those numbers are worth knowing, but they are not measuring the same event.
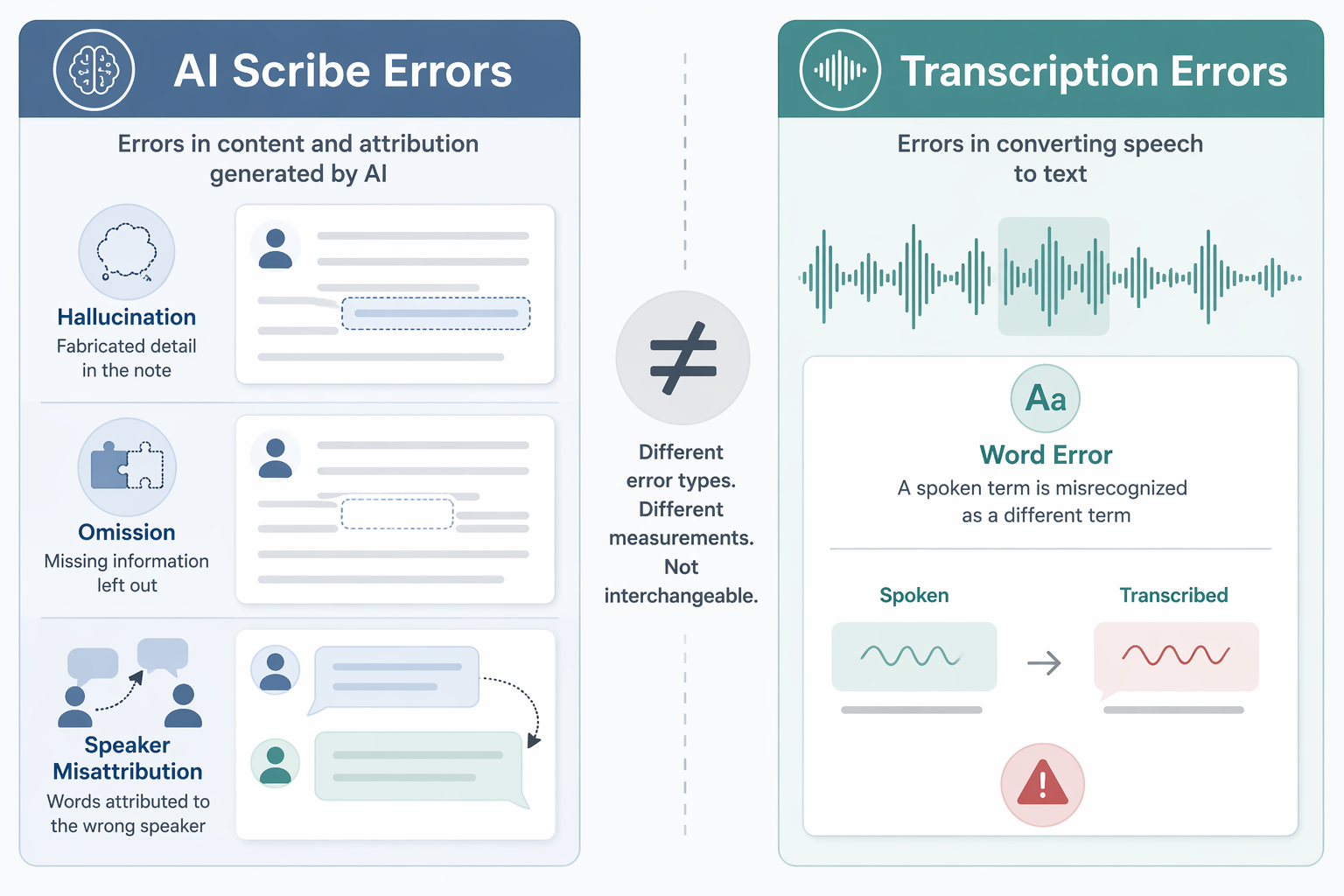
A word-error rate asks whether the recognized words match the spoken words. In transcription, that may mean a drug name, anatomical term, laterality, dosage, or abbreviation is misrecognized. The error can be obvious, or it can be clinically dangerous precisely because it looks ordinary inside a report.
An AI scribe error can be a different kind of failure. The note may add a detail that was not said, omit something important that was said, or assign a statement to the wrong speaker. Omission is especially uncomfortable because a missing negative, declined treatment, safety instruction, or follow-up condition may not call attention to itself. The clinician has to remember what is absent, not only notice what is wrong.
This distinction changes the review pattern. With transcription, the reviewer is often comparing the returned text against a dictated clinical narrative they intentionally created. With an AI scribe, the reviewer is comparing a synthesized note against a live encounter that may have included interruptions, patient questions, family members, side conversations, and non-linear clinical reasoning.
The same npj Digital Medicine commentary also flags equity concerns in speech recognition, including accuracy disparities for African American speakers.[3] That point belongs in this comparison because both pipelines depend on speech capture at some stage. Ambient documentation does not escape the old speech-recognition problem simply by adding a language model after it.
For a deeper safety-focused review of where ambient notes fail, see ClinicalMind's discussion of ambient AI scribe evidence and accuracy risks.
Where the Saved Time Goes
AI scribe vendors and adopters often lead with time savings, and there is real signal behind that interest. In a JAMA Network Open quality improvement study, clinician burnout decreased from 51.9% to 38.8% after 30 days of AI scribe use; the study reported 74% lower odds of burnout, but it used a pre-post design without a control group, so the finding should be read as an association rather than proof that the scribe caused the improvement.[4]
The Permanente Medical Group offers a larger operational example. Across 7,260 physicians and 2.5 million encounters, the organization reported 15,791 hours saved over 63 weeks, and 84% of physicians reported improved patient communication.[5] That scale is impressive because it reflects implementation in a real delivery system, not only a small pilot.
It still should not be pasted onto every clinic's business case. TPMG is a large, technologically mature system with the governance, training, and infrastructure to absorb a new documentation layer. A small multispecialty practice, a rural clinic, or a procedural group may see a different result. Some studies have found much smaller note-level savings, including only 34 seconds per note with high individual variability, which is a reminder that the time-savings story is not uniform.
The operational question is not only whether the draft arrives faster. It is whether the clinician spends less total time after review, correction, coding reconciliation, EHR navigation, and signature. A note that appears in seconds can still be expensive if it takes careful reconstruction to make it clinically and legally signable.
For readers focused specifically on burnout evidence, ClinicalMind has a separate synthesis of AI scribe burnout findings.
Cost Claims Need Attribution
AI scribe pricing is often presented as more predictable than transcription because many products use subscription models rather than per-line billing. A vendor-adjacent comparison from Healos states that AI scribes typically cost 30-60% less than transcription.[6] That figure is useful as a market claim, not as independent economic proof.
Actual cost depends on the contract, specialty, patient volume, note length, EHR integration, training, quality review, and whether the organization can retire any existing documentation expense. If an AI scribe subscription is added on top of retained transcription services, the cost comparison changes. If transcription is used only for high-value procedural reports while AI scribes cover high-volume outpatient visits, the blended model may make more sense than forcing one tool across every note type.
The Clinical Context Decides More Than the Technology

AI scribes fit best when the encounter itself contains the documentation raw material. Primary care, behavioral health, many specialty follow-ups, medication counseling, chronic disease management, and shared decision-making visits are plausible fits because the patient-clinician conversation carries the history, assessment, education, and plan.
In those visits, the value is not simply that the note is faster. It is that the clinician may be able to look up from the keyboard, maintain the conversation, and then edit a structured draft rather than build the note from scratch. That is the part of ambient documentation worth taking seriously.
Transcription remains well suited when the clinician's intended source is a dictated report. Operative reports, procedure notes, radiology interpretations, pathology reports, and other diagnostic narratives often require concise spoken detail from a clinician after the clinical work is complete. In those cases, there may be no meaningful ambient conversation to transform into a note, and a structured AI-generated visit note may be the wrong product.
The wrong implementation is easy to imagine. A practice buys an ambient tool because it worked in outpatient follow-up visits, then expects it to replace dictation for procedural documentation. The system may still produce text, but the missing ingredient is not model sophistication. It is the absence of the right input.
Governance Still Belongs in the Room
Many AI scribes are positioned as administrative tools rather than regulated medical devices, which creates a different oversight posture than software that directly diagnoses or treats disease.[3] That does not make them trivial. The signed note affects billing, continuity of care, malpractice exposure, quality reporting, and the patient's record.
A reasonable governance process should decide who can use the tool, which visit types are allowed, what consent language is required, how drafts are reviewed, how coding suggestions are handled, and how errors are reported. Those questions are not procurement paperwork. They define who bears the burden when the draft is wrong.
ClinicalMind's ambient AI scribe regulation article covers that oversight gap in more detail, and the implementation guide is the more practical next stop for teams already planning deployment.
A Fit Decision, Not a Winner
The best case for an AI scribe is a live clinical conversation that can be turned into a usable structured note with less after-hours composition and better patient-facing attention. The best case for transcription is a dictated clinical narrative where the clinician knows what needs to be said and the relevant facts are not naturally present in ambient room audio.
Both models can reduce typing. Both can introduce errors. Both leave the final responsibility with the clinician who signs the note. The defensible choice is not the newest pipeline or the most familiar one; it is the documentation method whose input, output, review burden, and failure modes match the clinical work being documented.
References
- Medical Transcription vs. AI Medical Scribes, Commure
- Traditional Medical Transcription vs AI Scribes, Freed
- Topaz et al. 2025 npj Digital Medicine commentary, npj Digital Medicine, 2025
- Ambient Artificial Intelligence Scribes and Physician Burnout, JAMA Network Open, 2025
- AI scribes save doctors 15,000 hours in documentation time, American Medical Association
- Medical Transcriptionist vs AI Medical Scribe, Healos
Comments
Join the discussion with an anonymous comment.