The Medicaid impact of the 2026 public charge rule is no longer a hypothetical compliance problem for immigrant healthcare access. DHS has rescinded the 2022 public charge regulation, removed the limiting “primarily dependent” standard, restored broader officer discretion, and again allows immigration officers to consider Medicaid, CHIP, SNAP, housing assistance, and other noncash benefits when making public charge inadmissibility determinations. USCIS announced the rescission of the 2022 regulation, and the final rule is effective September 18, 2026 unless litigation changes that timetable.[1]
That is the operational change. It means the front desk, call center, eligibility office, pediatric clinic, and hospital finance department now have to work inside a discretion-heavy framework that many families will hear as a warning: using health coverage could hurt an immigration case. The legal reality is narrower than that sentence. The behavioral effect is not.

What changed in 2026
The mechanics matter because public charge is not a general benefit ban. It is an inadmissibility ground: a forward-looking judgment about whether a person is likely to become dependent on government support. The 2026 rule changes how that judgment is made. By rescinding the 2022 definitions, DHS no longer confines public charge analysis to a narrower set of benefits or to the idea that a person must be “primarily dependent” on government assistance before benefit use carries weight.[1]
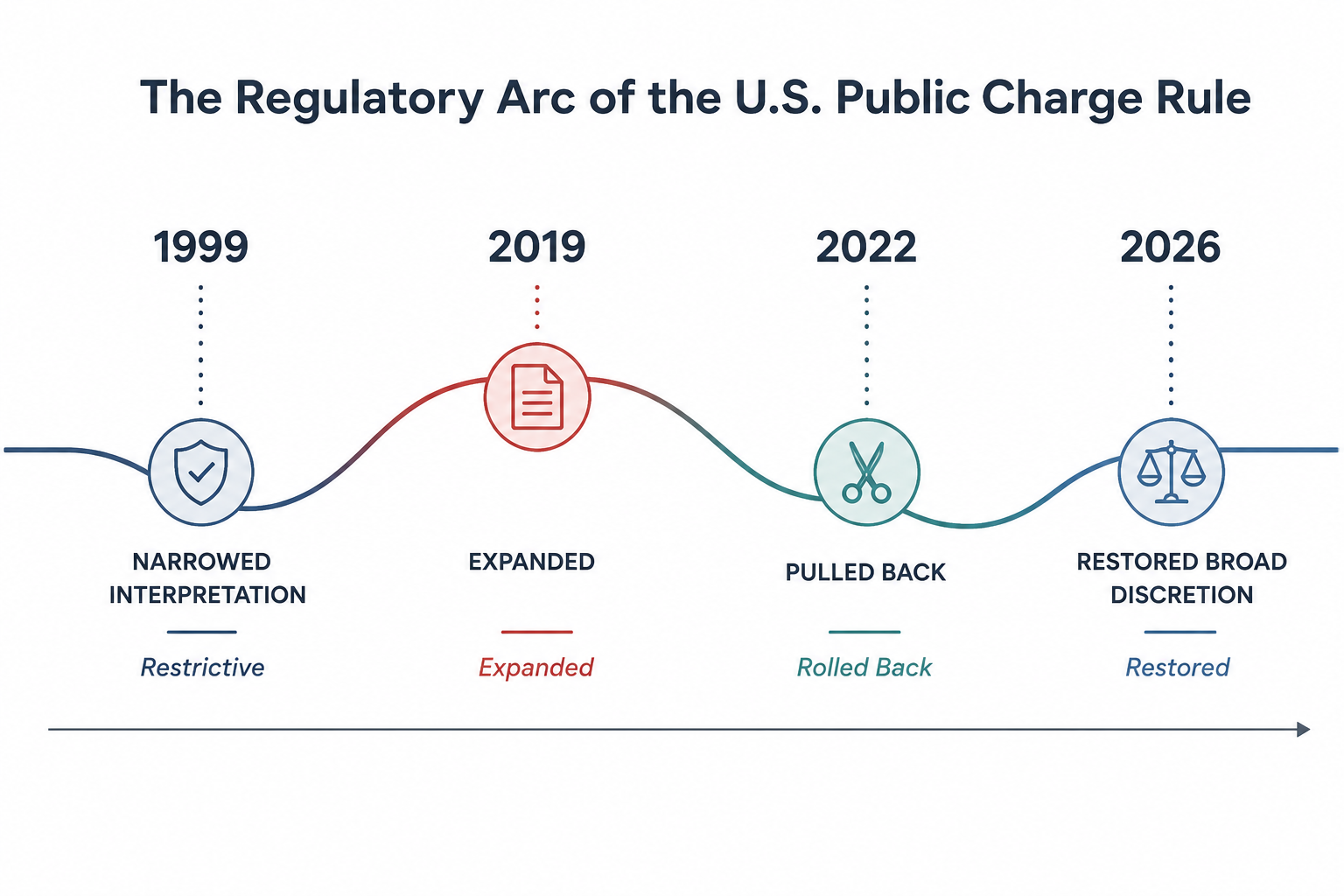
The practical arc is short but important. In 1999, federal guidance narrowed the working interpretation of public charge in a way that generally excluded most noncash benefits from consideration. In 2019, the Trump administration expanded the rule and sharply increased the benefit categories and personal factors officers could weigh. In 2022, the Biden administration pulled the policy back. In 2026, DHS has restored a broader discretion model.[2]
That sequence is why the 2026 rule should not be treated as a technical cleanup. A change in definitional scope changes what an officer may weigh. A change in officer discretion changes what lawyers, navigators, and community organizations feel safe saying. A change in what those trusted messengers say changes whether families renew Medicaid or CHIP.
| Policy point | Operational meaning for health coverage |
|---|---|
| 2022 definitions rescinded | Prior narrowing no longer controls the public charge framework |
| “Primarily dependent” standard eliminated | Officers are not limited to asking whether a person is mainly dependent on public benefits |
| Medicaid and other noncash benefits may be weighed | Families may avoid or drop coverage even when eligibility technically remains |
| Effective date set for September 18, 2026 | Health systems have a short window to update scripts, training, and referral workflows |
Direct legal exposure is narrower than the fear it creates
The first mistake in explaining public charge is to imply that every immigrant enrolled in Medicaid is directly exposed in the same way. Public charge inadmissibility does not apply to every immigration status, every application, or every family member. It is not a retroactive punishment for everyone who ever used a benefit. It is a discretionary admissibility analysis applied in specific immigration contexts.
The second mistake is to stop there. In clinics, a legally precise reassurance often arrives after the damage has already been done. A parent hears that Medicaid can be considered. A cousin says SNAP renewal could be risky. A front-desk worker, worried about giving immigration advice, says the family should talk to a lawyer before continuing coverage. The renewal notice sits untouched. The child misses a well visit. The hospital sees the patient later, sicker and uninsured.

That is the spillover channel: the rule applies to admissibility determinations, but enrollment behavior changes in households. Mixed-status families do not sort regulatory categories at the kitchen table the way agencies sort them in the Federal Register. A citizen child may remain fully eligible for Medicaid or CHIP, while a noncitizen parent still decides that any government-program interaction feels unsafe.
The disenrollment estimates are large, but they are not the same estimate
DHS’s own impact analysis gives the first anchor. The agency projected a 10.3% disenrollment rate, affecting about 422,748 people. It also estimated roughly $9 billion in annual federal and state transfer-payment reductions, with $5.76 billion, or 65%, tied to Medicaid and CHIP coverage losses.[3]
Those figures should be read carefully. A transfer-payment reduction is not a savings estimate in the way a hospital CFO would use the word. It means fewer public dollars flowing through coverage programs. Some of the foregone care disappears. Some becomes delayed care. Some returns as bad debt, charity care, uncompensated emergency department use, or avoidable deterioration.
KFF’s independent analysis produces a wider and larger range: 1.3 million to 4.0 million Medicaid and CHIP disenrollments, including 600,000 to 1.8 million citizen children. KFF’s range uses 10% to 30% chilling-effect assumptions, drawing from prior public charge experience rather than DHS’s narrower 10.3% assumption.[3]
| Estimate | Projected Medicaid/CHIP effect | What drives the difference |
|---|---|---|
| DHS impact analysis | About 422,748 disenrollees at a 10.3% rate | Narrower assumed disenrollment response |
| KFF analysis | 1.3 million to 4.0 million disenrollees | 10% to 30% chilling-effect assumptions based on prior experience |
| KFF citizen-child subset | 600,000 to 1.8 million citizen children | Household spillover among children whose own eligibility may remain intact |
The gap between 422,748 and 4.0 million is not a rounding dispute. It is a disagreement over behavior under fear, confusion, and uneven outreach. DHS is estimating one response level. KFF is testing a broader range because the 2019 episode showed that public charge anxiety can move far beyond the population directly subject to the rule.
The most striking part of the official analysis is not only the enrollment projection. DHS acknowledged that the rule may lead to worse health outcomes, increased emergency room use, higher prevalence of communicable diseases, and increases in uncompensated care.[3] That list is the bridge from immigration regulation to healthcare operations.
The 2019 rule is the plausibility test
The reason a large chilling effect is plausible is that the country has seen one. Migration Policy Institute analysis found that the 2019 rule increased the share of noncitizens subject to public charge determinations from about 3% to about 47%. The same analysis reported that Medicaid participation fell 20% among low-income noncitizens.[4]
That does not prove the 2026 effect will land at the top of KFF’s range. The policy environment is different, state outreach varies, litigation could interrupt implementation, and some families may have clearer information than they had in 2019. But the 2019 data make it hard to dismiss the larger range as speculative panic. When eligibility workers tell stories about families withdrawing from programs they were still allowed to use, those stories now sit inside an empirical pattern, not outside it.
Children show why the direct-eligibility lens is too narrow. Georgetown’s Center for Children and Families has warned that public charge changes can reach children, pregnant women, and families through fear and household-level decision-making.[5] An AAP Pediatrics article reported that during the 2019 rule period, Medicaid and CHIP participation fell 18% among citizen children in noncitizen households, compared with 8% among citizen children in citizen-only households.[6]
That comparison is hard to explain away as ordinary Medicaid churn. It points to a specific behavioral spillover: children who are citizens, and therefore not themselves public charge applicants, losing coverage at higher rates because adults in the household perceive risk.
Fear did not disappear when the 2019 policy was reversed
One reason health systems should not expect a clean reset is that public charge fear persisted after the 2021 reversal of the 2019 rule. Urban Institute data showed that 14% of adults in immigrant families with children avoided safety-net programs in 2022–2023.[7] KFF reported that in 2023, 16% of adults in immigrant families still incorrectly believed use of public programs would affect green card status.[8]
That persistence matters for 2026 implementation. A family that avoided Medicaid in 2022 because of a repealed rule may not parse a new final rule with confidence. A navigator who spent years saying “the 2019 rule no longer applies” now has to explain a new rule that restores broader discretion without overstating who is directly affected. That is a difficult script even for trained staff.
The current fear environment is already elevated. In the 2025 KFF/New York Times Survey of Immigrants, 29% of immigrants reported skipping or postponing care, 11% said they had stopped participating in assistance programs since January 2025, 41% said they worried about detention or deportation, and 51% said they were concerned about data sharing.[9]
The CMS–ICE Medicaid data-sharing agreement intensifies that problem. Even where coverage rules remain unchanged, families may treat Medicaid enrollment information as a potential immigration-enforcement risk. For public charge implementation, that means the behavioral baseline is not neutral. The rule arrives in a year when many immigrant families are already questioning whether healthcare access creates a record that can be used against them.[9]
How the rule becomes visible inside healthcare
Hospitals and clinics will not see “public charge” as a single line item. They will see it in missed renewals, more uninsured visits, higher self-pay balances, children falling out of managed-care attribution, and patients arriving later in the disease course. The first operational signs are likely to appear before the effective date if families and community messengers react to the rule’s publication itself.
- Enrollment avoidance: eligible families decline new Medicaid or CHIP applications because the household cannot distinguish eligibility from immigration risk.
- Renewal attrition: families already enrolled fail to complete redetermination paperwork after hearing that benefits may be considered.
- Delayed care: patients postpone primary care, prenatal care, behavioral health visits, prescriptions, or specialty follow-up until symptoms become harder to ignore.
- Emergency department substitution: care shifts from covered outpatient settings to higher-cost urgent or emergent encounters.
- Uncompensated care growth: coverage losses reappear as charity care, bad debt, and pressure on safety-net providers.
DHS’s own impact statement names several of these consequences, including worse health outcomes, increased emergency room use, communicable disease risk, and uncompensated care.[3] That admission should shape how health systems prepare. The issue is not only whether a patient is correctly advised about public charge on a given day. It is whether the institution can prevent a generalized fear of coverage from becoming a utilization pattern.
The timing also overlaps with other coverage changes. Commonwealth Fund analysis of 2025 reconciliation-law changes reported that about 1 million lawfully present immigrants could lose coverage access beginning in October 2026.[10] Public charge implementation is scheduled for September 18, 2026, which means coverage offices may be explaining public charge, Medicaid eligibility restrictions, and immigration-data concerns in the same season.
What health systems should watch before September
The exact enrollment loss is not knowable in July 2026. Litigation could stay or narrow the rule before September 18. Subregulatory guidance could clarify how officers should weigh different benefits. State Medicaid agencies and community organizations could blunt some of the chilling effect with precise outreach. Or confused messaging could magnify it.
For healthcare organizations, the useful work is not to guess one final national number. It is to monitor the points where fear becomes measurable.
- Medicaid and CHIP renewal completion among households with preferred languages other than English.
- Self-pay visits and bad-debt trends in clinics serving large immigrant communities.
- No-show rates for pediatric, prenatal, chronic-disease, and behavioral-health appointments.
- Call-center questions about whether Medicaid, CHIP, SNAP, or housing assistance can affect immigration status.
- Referrals from eligibility staff to legal-aid partners, especially when families withdraw applications before completing screening.
Training should separate legal exposure from household fear. Staff need enough precision to avoid saying that all benefit use is dangerous, and enough humility to avoid giving immigration advice outside their role. The safest operational model is usually a tight script, a current benefits chart, documented referral pathways to qualified immigration counsel, and multilingual materials that explain which household members and application types may be affected.
The restored discretion framework is likely to produce a large chilling effect on Medicaid and CHIP participation among immigrant families. DHS’s 422,748 projection and KFF’s 1.3 million to 4.0 million range should both remain on the table because they answer the same question with different assumptions about fear. The final magnitude will depend less on statutory eligibility alone than on litigation, agency guidance, outreach quality, and whether families believe health coverage information will not be used against them.
References
- US Citizenship and Immigration Services Rescinds 2022 Public Charge Regulation, USCIS
- Explainer: 2025 Proposed Rule on Public Charge, National Immigration Forum
- Potential Chilling Effects of Public Charge and Other Immigration Policies on Medicaid and CHIP Enrollment, KFF
- Anticipated “Chilling Effects” of the Public-Charge Rule Are Real: Census Data Reflect Steep Decline in Benefits Use by Immigrant Families, Migration Policy Institute
- Public Charge Changes Will Have Far-Reaching Consequences for Children, Pregnant Women, and Families and Sow Fear in Immigrant Communities, Georgetown University Center for Children and Families, November 21, 2025
- Public Charge Rule and Its Impact on Child Health, Pediatrics
- One in Six Adults in Immigrant Families with Children Avoided Public Programs in 2022, Urban Institute
- Changes to Public Charge Regulations Will Likely Lead More Immigrant Families to Avoid Health Care and Assistance Programs, KFF
- Potential Implications of the New Medicaid Data Sharing Agreement Between CMS and ICE, KFF
- What Recent Policy Changes Mean for Immigrant Health Coverage, Commonwealth Fund, October 2025
Comments
Join the discussion with an anonymous comment.