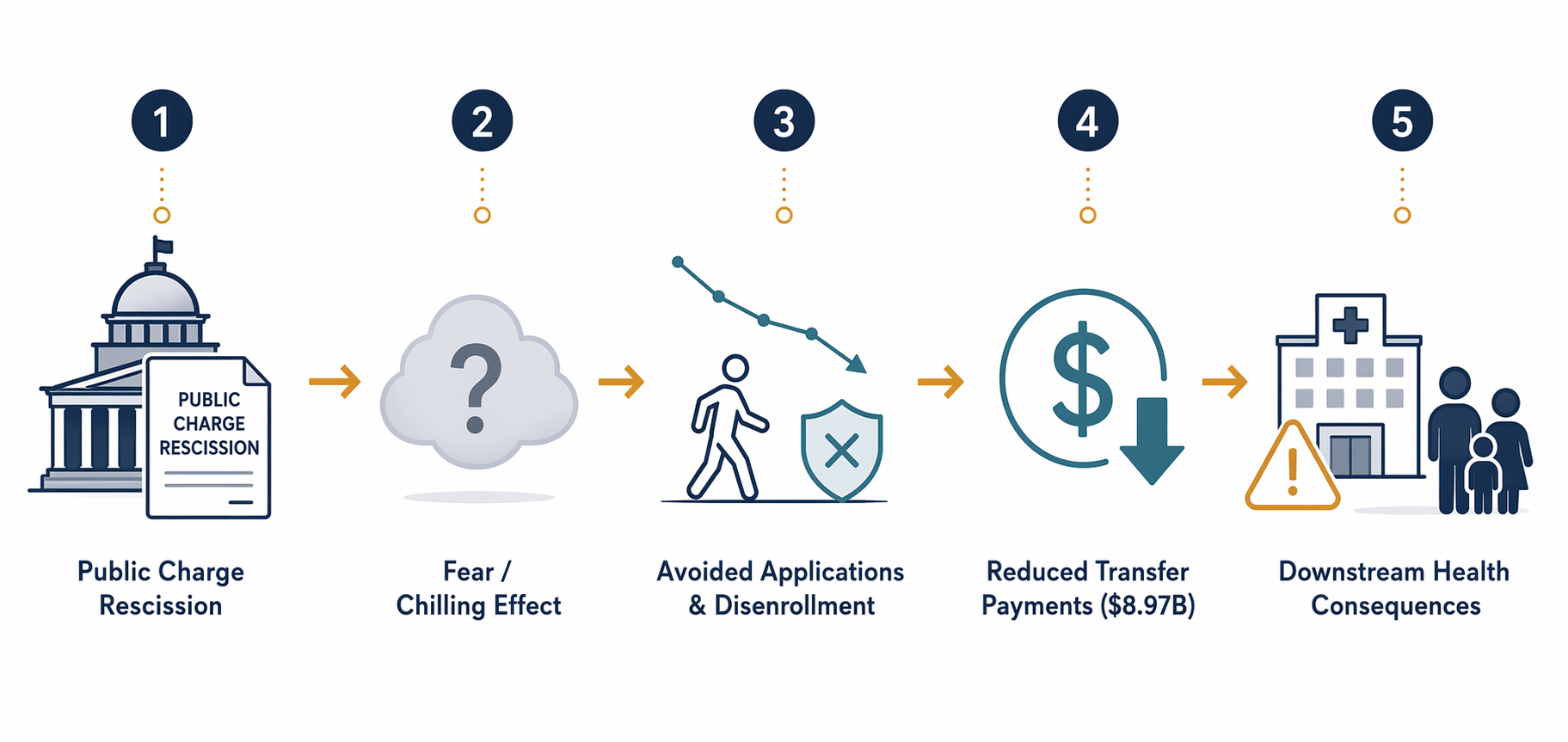
The useful starting point for the 2026 public charge rule is not the phrase “green card denial,” even though that is where most families will hear the warning. The larger Medicaid and food stamps problem is behavioral: people who remain legally eligible for Medicaid, CHIP, SNAP, or housing assistance decide that applying is too risky, renewing is too exposed, or keeping a child enrolled is not worth the chance that an immigration officer could later treat the household’s records unfavorably.
DHS put numbers on that behavior in its own regulatory analysis. In the November 2025 proposed rule rescinding the 2022 public charge regulation, the agency modeled disenrollment scenarios of 3.3 percent, 10.3 percent, and 17.3 percent among people affected by the chilling effect. At the 10.3 percent midpoint, DHS estimated $5.29 billion in reduced federal transfer payments and $3.68 billion in reduced state transfer payments annually, or $8.97 billion combined each year.[1]
That is the figure to hold onto. It is not an outside advocate’s worst case. It is the agency’s own midpoint estimate of dollars no longer moving through Medicaid, CHIP, SNAP, and related programs because people are expected to leave or avoid benefits.
DHS’s midpoint is large, and its range is doing real work
Budget staff tend to distrust single-point estimates because the reconciliation always arrives later. DHS’s analysis gives a midpoint, but it also shows why the midpoint should not be mistaken for precision. The agency modeled a low scenario of 3.3 percent disenrollment, a midpoint of 10.3 percent, and a high scenario of 17.3 percent. It also acknowledged that the 10.3 percent assumption “could be influenced by external factors unrelated to this proposed rule” and “may be an underestimate or an overestimate.” Studies cited in the rule ranged more widely, from 3.3 percent to 48 percent, depending on methodology and population.[1]
| DHS scenario | Disenrollment assumption | What it means for planning |
|---|---|---|
| Low | 3.3% | A measurable reduction, but one that may be absorbed unevenly across states, eligibility groups, and local providers. |
| Midpoint | 10.3% | $8.97 billion in annual federal and state transfer payment reductions across affected programs. |
| High | 17.3% | A materially larger access and utilization shock, especially where immigrant families are concentrated. |
The uncertainty does not make the estimate unusable. It tells state agencies and health systems what kind of uncertainty they are dealing with. The question is less whether the direction of movement is plausible than whether the local effect looks like drift, a program integrity-looking renewal dip, or a concentrated coverage loss among households that were already less likely to seek care early.
The final rule was announced by USCIS on July 16, 2026, with an effective date of September 18, 2026. As of July 18, 2026, the final Federal Register text had not yet published; USCIS said publication would occur on July 20, 2026. That matters because the exact sub-regulatory guidance has not yet been released, and litigation could still alter timing or implementation.[2]
The coverage-loss check: Georgetown’s Medicaid and CHIP estimate
Georgetown’s Center for Children and Families applied DHS’s 10.3 percent midpoint to Medicaid and CHIP and estimated 422,748 coverage losses. Of those, 58,747 were CHIP enrollees, meaning children or pregnant women.[3]
That number is useful because it narrows the big DHS transfer-payment estimate into a program population Medicaid offices can recognize. It is not the entire universe of people affected by the rescission. It is a modeled Medicaid and CHIP loss using DHS’s midpoint assumption. But it helps translate the $8.97 billion midpoint into renewal queues, managed care capitation movement, pediatric appointment gaps, and uncompensated-care exposure.
It also keeps the analysis from sliding into the wrong denominator. Public charge inadmissibility decisions formally apply to certain noncitizens seeking admission or adjustment to lawful permanent resident status. The chilling effect reaches a much larger administrative surface: households where one person’s immigration concern changes another person’s benefit decision.
The affected household is not always the applicant
KFF estimated that 13.4 million Medicaid and CHIP enrollees lived in a household with a noncitizen as of 2023. That is the population exposed to confusion, caution, rumors, legal advice, and family-level risk calculations, even though not every person in those households is personally subject to a public charge determination.[4]
This is where a formal green card denial frame becomes too narrow. A U.S. citizen child cannot be denied a green card because the child used Medicaid. But a parent can still decide that the safest move is to avoid the county office, skip a renewal, or let SNAP lapse because the household cannot confidently separate one family member’s eligibility from another family member’s immigration file.

Urban Institute findings cited in the policy literature point in the same direction. In 2022–2023, 25 percent of adults in mixed-status families avoided noncash government benefits because of green card concerns, compared with 7 percent in all-citizen families.[3] That difference is not a denial rate. It is a household behavior rate, and for Medicaid financing it is often the behavior rate that shows up first.
Avoidance was already measurable before the 2026 effective date
The survey evidence does not prove how many people will disenroll after September 18. It does show that the mechanism DHS modeled already exists. In a 2025 KFF/New York Times survey, 12 percent of immigrant adults said they avoided applying for assistance programs in the prior year, up from 8 percent in 2023. The same survey found that 29 percent skipped or postponed health care.[5]
The parent-specific numbers are more operationally uncomfortable. KFF reported that 18 percent of immigrant parents avoided applying for assistance programs, up from 11 percent in 2023, and 17 percent had stopped participating in programs since January 2025.[5]
For a Medicaid agency, those figures are not just attitudes. They can become lower application volume, nonresponse to renewal packets, increased churn, delayed prenatal entry, and children reappearing at the point of care without active coverage. For a hospital system, they can become a payer mix issue before anyone has a clean legal answer about how many inadmissibility findings the rule will actually produce.
The transfer-payment reduction is not a savings story
DHS did not present the $8.97 billion annual reduction as a tidy benefit. The agency framed the federal and state transfer-payment reductions as costs. That distinction matters. In a Medicaid forecast, reduced spending caused by eligible people leaving coverage is not the same thing as utilization management, lower acuity, better care coordination, or fewer eligible residents. It is a reduction in public support caused by changed behavior.[1]
The accounting pathway is straightforward enough to model and hard enough to manage: rescission changes the perceived risk of benefit use; some households avoid or drop Medicaid, CHIP, SNAP, or other noncash benefits; federal and state transfer payments decline; health systems and local agencies see the downstream costs in different ledgers. A Medicaid line item may fall while emergency departments, safety-net clinics, public health programs, and school-linked supports absorb more of the practical consequence.
The rule’s effect will not distribute evenly. Counties with large mixed-status households, states with higher immigrant enrollment in Medicaid and CHIP, and providers serving pregnant women and children are more likely to see the signal. Some of it may be misread at first as ordinary redetermination friction or outreach fatigue. That is why the timing matters: if declines cluster after the rule’s effective date, the cleaner budget explanation may not be the correct operational explanation.
DHS also names the health harms
The downstream consequences are not speculative add-ons from outside commentators. DHS itself said the proposed rule may lead to “worse health outcomes, increased use of emergency rooms, higher prevalence of communicable diseases, increased poverty, housing instability, and reduced educational attainment.” The agency also identified increased prevalence of obesity and malnutrition, especially among pregnant or breastfeeding women, infants, and children, and reduced prescription adherence.[1]
Those are broad harms, but the operational channels are familiar. SNAP loss can change food security before a health claim appears. Medicaid loss can interrupt prescriptions before an inpatient event. CHIP loss can delay routine pediatric care until a school nurse, urgent care clinic, or emergency department becomes the point of contact. Housing assistance avoidance can make address instability worse, which then makes Medicaid renewal mail and managed care outreach less reliable.
None of that requires every affected person to receive a green card denial. In fact, the main fiscal and health effect DHS modeled is not a pile of denial notices. It is the quieter disappearance of participation by people who may still qualify.
No bright line means more conservative household decisions
Legal uncertainty does not sit outside the enrollment analysis; it feeds the enrollment analysis. Migration Policy Institute warned that the proposed rule leaves open the possibility that use of programs such as Head Start, free school lunch, care at Community Health Centers, or other services could hurt future green card applications because no bright-line rule exists.[6]
That kind of ambiguity changes the household calculation. A family rarely parses regulatory categories the way counsel, agencies, or policy shops do. If the perceived rule is “benefits may count,” the practical response can be to avoid more than the formal rule requires. That is how a policy aimed at public charge determinations can reach citizen children, pregnant women, and other household members who are absent from the headline version.
This is also where implementation guidance will matter. USCIS has announced the rescission and the effective date, but the precise sub-regulatory guidance was not yet available as of July 18, 2026.[2] If guidance later narrows or clarifies how officers treat specific benefits, that could affect the size of the chilling effect. If guidance leaves broad discretion in place, households may continue to behave as though the safest option is nonparticipation.
Litigation is a timing risk, not a reason to ignore the signal
The 2026 rule is likely to face legal challenges, and a court could delay or block implementation. The prior public charge fight showed how quickly litigation can alter operational timelines. For planning purposes, that creates a brake on overconfident forecasting, especially because the final Federal Register text and later guidance may differ in material ways from the November 2025 proposal.
But litigation risk does not erase the behavior already measured in surveys or the agency’s own expectation of reduced participation. Families do not always wait for injunctions, final manuals, or FAQs. Some act on news coverage, community warnings, legal uncertainty, or past experience with immigration policy. That is one reason chilling effects can begin before an effective date and continue even when the legal status becomes more complicated.
What administrators and providers should watch
The cleanest monitoring question is not whether the public charge rule caused every individual disenrollment. It is whether the post-rule pattern differs from expected renewal behavior, especially among households likely to include noncitizens. Agencies and providers will need to separate ordinary eligibility losses from nonresponse, fear-driven withdrawal, and avoided applications.
- Application volume for Medicaid, CHIP, SNAP, and pregnancy-related coverage in communities with high mixed-status household exposure.
- Renewal nonresponse and procedural termination patterns after the September 18, 2026 effective date, if implementation proceeds.
- Pediatric and prenatal coverage gaps, especially where CHIP and pregnancy-related Medicaid have historically carried stable enrollment.
- Emergency department utilization and uncompensated-care changes among patients who previously had Medicaid or CHIP coverage.
- Call-center, navigator, and eligibility-worker questions that show whether families are avoiding benefits beyond those actually implicated by the rule.
The last item is easy to undervalue because it does not arrive as a claim. It arrives as confusion: a parent asking whether a citizen child’s Medicaid renewal could hurt a spouse, a pregnant woman declining help until after delivery, a family dropping SNAP but keeping a clinic appointment, or a household changing its mailing address and then disappearing from the renewal cycle.
The defensible conclusion is about direction
The exact magnitude of the 2026 public charge rescission will depend on the final text, USCIS guidance, litigation, outreach, state enrollment systems, and how much families trust reassurances from agencies and providers. DHS’s midpoint could be too high or too low. The range around it is wide enough that anyone building a forecast should carry more than one scenario.
The direction is much harder to dismiss. DHS expects disenrollment and forgone enrollment large enough to reduce federal and state transfer payments by billions of dollars annually at the midpoint. KFF survey data show avoided applications and postponed care were already occurring. Georgetown’s Medicaid and CHIP estimate gives a concrete scale check for coverage losses. The households most likely to absorb the first hit are immigrant families and citizen children in mixed-status homes; the institutions most likely to see it early are clinics, hospitals, state eligibility systems, and public programs that will be reconciling the numbers while the legal fight is still moving.
References
- Public Charge Ground of Inadmissibility, Federal Register, November 19, 2025.
- U.S. Citizenship and Immigration Services Rescinds 2022 Public Charge Regulation, USCIS.
- Public Charge Changes Will Have Far-Reaching Consequences for Children, Pregnant Women and Families and Sow Fear in Immigrant Communities, Georgetown Center for Children and Families, November 21, 2025.
- Potential Chilling Effects of Public Charge and Other Immigration Policies on Medicaid and CHIP Enrollment, KFF.
- Changes to Public Charge Regulations Will Likely Lead More Immigrant Families to Avoid Health Care and Assistance Programs, KFF.
- Trump Administration Public-Charge Rule Would Amplify Harms to Immigrant Families, Migration Policy Institute, November 2025.
Comments
Join the discussion with an anonymous comment.