For anyone searching for TrumpRx drug discount program coverage and eligibility, the current answer is narrower than the public branding suggests. As of July 18, 2026, TrumpRx functions as a cash-pay discount portal, not as health insurance coverage. It is designed around discounted prices for listed drugs, but it does not create a pharmacy benefit, does not replace a plan formulary, and does not automatically fit into Medicare, Medicaid, employer coverage, or Affordable Care Act marketplace coverage.
The White House launched TrumpRx.gov in February 2026 as a program intended to bring lower prescription drug prices to patients, presenting it as part of a broader effort to secure most-favored-nation-style pricing and claiming $400 million in savings through manufacturer agreements.[1] The practical eligibility rules, however, do most of the work. KFF’s analysis describes a program that can help some people in some transactions, while excluding large insured groups and leaving others to decide whether a cash price outside insurance is worth the tradeoff.[2]
Who Can Use TrumpRx Today
The cleanest way to understand TrumpRx eligibility is to separate the ability to buy a drug at a listed cash price from the ability to use insurance. TrumpRx is built for cash payment. That means the patient pays the discounted TrumpRx price directly rather than running the purchase through a health plan’s pharmacy benefit.
| Patient or coverage status | Current TrumpRx access | Main practical consequence |
|---|---|---|
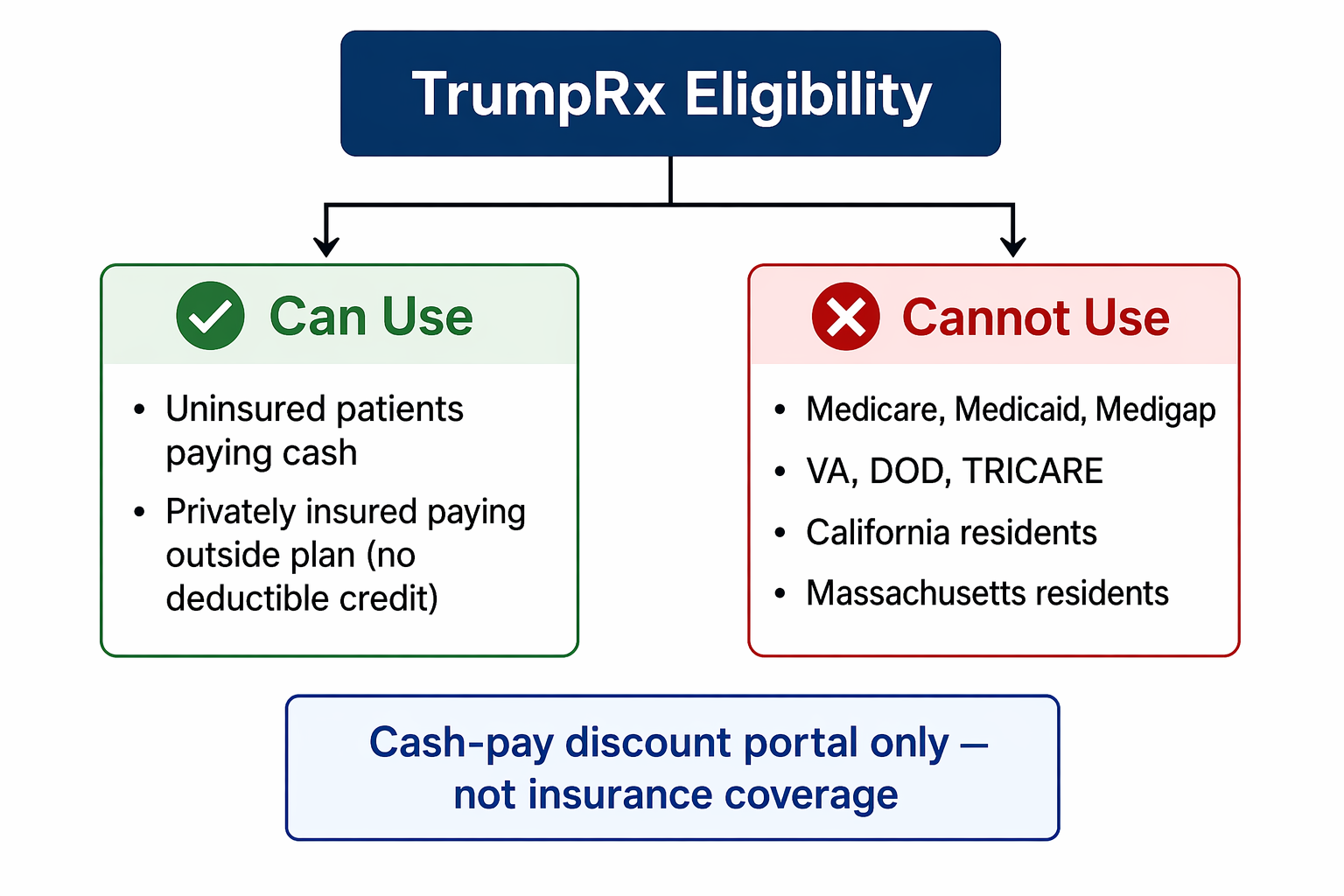
| Uninsured patient | Can use TrumpRx if the drug is listed and state restrictions do not apply | Pays the cash price; no insurance benefit is involved |
| Privately insured patient | Can choose to pay cash outside the plan | The purchase generally does not count toward the plan deductible or out-of-pocket maximum |
| Medicare, Medicaid, Medigap, VA, DOD, or TRICARE beneficiary | Cannot use TrumpRx | Must rely on existing coverage or other lawful payment channels |
| Resident of California or Massachusetts | Blocked from using the program | State availability removes access regardless of otherwise eligible status |
Each line of that table matters. An uninsured patient is the most straightforward user: if the drug appears on TrumpRx, the patient is not in an excluded state, and the discounted cash price is still affordable, the program may create a real savings opportunity. That is not a small thing for the right patient on the right medicine.
The privately insured patient has a more complicated choice. A person with employer coverage or individual-market coverage may be able to pay the TrumpRx cash price, but that is a purchase outside the plan. KFF notes that such payments do not count toward the patient’s deductible or out-of-pocket maximum under current rules.[2] In plain terms: the patient may save money at the counter today, but the health plan will usually act as though that spending never happened.
That matters most for patients who expect substantial prescription or medical spending later in the year. A $100 cash purchase can look better than a $160 plan price in isolation. But if the $160 would have moved the patient closer to satisfying a deductible or annual out-of-pocket limit, the cheaper cash transaction may have a hidden cost. The right comparison is not just TrumpRx versus the pharmacy counter price; it is TrumpRx versus the patient’s year-long benefit design.
The Public Insurance Exclusion Is Not a Fine Print Detail
TrumpRx excludes people covered by Medicare, Medicaid, Medigap, VA, DOD, and TRICARE programs.[2] That means the program is not an alternate federal drug benefit for seniors, low-income Medicaid beneficiaries, veterans, military families, or other public-program enrollees. Those groups are not merely less advantaged by the program; they are outside its eligibility boundary.
This is where loose use of the word “coverage” becomes expensive. A Medicare patient who hears that a federal drug discount program exists may reasonably assume there is a Medicare pathway into it. For TrumpRx, that assumption is wrong. The program may carry federal branding, but public insurance beneficiaries are excluded under the eligibility rules described by KFF and launch reporting.[2][3]
Clinic staff, pharmacists, and benefits teams will feel this distinction at the counter. The patient’s question will be simple: can I use TrumpRx for this drug? For a Medicare, Medicaid, Medigap, VA, DOD, or TRICARE beneficiary, the answer is no, even before price comparison begins.
Private Insurance Users Face a Tradeoff, Not a New Benefit
For privately insured patients, TrumpRx is best understood as an outside-the-plan cash option. That option may be rational in some cases. If a listed drug has a high plan cost-sharing amount, is not covered, or is subject to a formulary barrier, a discounted cash price may be attractive. But the patient is stepping away from the plan’s accounting system when using the TrumpRx price.
The deductible issue deserves translation. A deductible is the amount a patient must pay before certain insurance benefits begin. An out-of-pocket maximum is the annual ceiling after which covered in-network care generally becomes much less expensive for the patient. When a TrumpRx cash purchase does not count toward either amount, the patient may still have to spend the same deductible dollars later through the insurance plan.
Aon’s employer advisory treats this as a plan-sponsor issue rather than just a consumer shopping issue, because employers and benefit administrators may need to explain why a visibly lower cash price does not necessarily integrate with the employee’s health plan.[4] That is the right frame. The problem is not that cash discounts are inherently bad; the problem is that a cash discount and an insured pharmacy claim solve different problems.
There is one possible future caveat, but it should not be mistaken for current functionality. Aon notes that a February 2026 FTC settlement involving Express Scripts included a provision that could allow TrumpRx payments to count toward deductibles “upon relevant legal and regulatory changes.”[4] As of July 2026, that condition has not been implemented. For today’s patient, the safer operational assumption is that TrumpRx cash spending remains outside normal deductible and out-of-pocket maximum accumulation.
State Availability Narrows the Funnel Further
Eligibility also depends on geography. TrumpRx is unavailable to residents of California and Massachusetts, which KFF identifies as affecting about 46 million Americans.[2] That restriction is not a marginal footnote. It removes two large states from the program’s practical reach, regardless of whether a patient is uninsured or otherwise willing to pay cash.
For national employers, health systems, and patient assistance teams, that creates a communication problem. A patient in Nevada and a patient in California may have the same drug, the same uninsured status, and the same financial need, but only one may be able to use the portal. Any eligibility explanation that stops at “uninsured patients can use it” is incomplete.
Drug Coverage Is Growing, But Still Hard to Treat as Broad Coverage
The drug list is another reason the word “coverage” needs care. At launch in February 2026, TrumpRx covered 43 drugs. By April 2026, the list had grown to 80 drugs, which KFF described as about 0.3% of FDA-approved drugs.[2] That is a limited starting point for any patient or clinician trying to understand whether the program is likely to matter in routine care.
The administration announced a larger expansion in May 2026, saying the program would move toward more than 800 medications, including generics.[5] That announcement may become important, but as of July 18, 2026, the final confirmed scope and pricing of that expansion should be treated cautiously unless the specific drug and price are visible to the patient at the time of purchase.
A narrow list can still help if it contains the patient’s medication. But a portal with dozens or even hundreds of drugs is not the same thing as a plan formulary. Insurance formularies are embedded in coverage rules, pharmacy networks, utilization management, deductible structures, and annual spending limits. TrumpRx is closer to a publicly branded cash-price marketplace for selected drugs. That distinction may sound technical until a patient’s medication is not on the list.
The selection logic also raises fair questions. KFF noted that nelfinavir, an HIV drug that NIH recommends against, appeared on the TrumpRx list.[2] One listing does not prove a broader pattern, but it does show why the drug list should be evaluated by current clinical relevance as well as by the number of products displayed.
Discounted Does Not Always Mean Affordable
The program’s strongest case is the uninsured patient who needs a listed drug and can pay the discounted amount. That is a real group, and it should not be waved away. Cash discounts can matter when the alternative is a higher retail price or no purchase at all.
But uninsured eligibility is not the same as uninsured affordability. KFF notes that nearly half of uninsured Americans have incomes below 200% of the federal poverty level.[2] For many of those patients, a lower cash price may still be out of reach, especially for chronic therapies, specialty drugs, or households already rationing care.
This is the gap that headline savings claims often skip. A patient does not benefit from a discount simply because the discount exists. The patient benefits only if the drug is included, the patient is eligible, the state allows access, the price is lower than available alternatives, and the remaining cash amount can actually be paid.
The Savings Claim Needs a Narrow Reading
The White House presented TrumpRx as a major drug-pricing initiative tied to confidential manufacturer agreements and a most-favored-nation pricing agenda.[1] The broader policy frame traces to Executive Order 14297, issued in May 2025, which directed efforts to deliver most-favored-nation prescription drug pricing to American patients.[6]
Confidential agreement terms make full outside verification difficult. KFF notes that the specific terms of the 15 manufacturer agreements were not public, limiting the ability to validate broad savings claims across the program.[2] That does not mean every price is meaningless. It means the advertised program-level savings should not be treated as a patient-specific estimate.
Comparisons with existing cash-price tools complicate the value claim further. The Center for American Progress, in a corrected April 2026 analysis, found that only 31 of the 80 TrumpRx drugs offered savings not already available through GoodRx or Cost Plus Drugs.[7] That finding does not eliminate TrumpRx’s usefulness for those 31 drugs, but it does narrow what the program can claim as distinctive value.
For a patient, the practical question is not whether TrumpRx is cheaper than an abstract list price. It is whether TrumpRx is cheaper than the price the patient could actually obtain through insurance, a manufacturer assistance channel, GoodRx, Cost Plus Drugs, a pharmacy discount card, or another lawful cash-pay option. That comparison will vary by drug and by patient.
What Coverage Means Here
If “coverage” means the existence of a public-facing portal with discounted prices on selected drugs, then TrumpRx has coverage. If “coverage” means an insured pathway that a patient can use through Medicare, Medicaid, VA, TRICARE, or a private plan while preserving normal benefit credit, then TrumpRx does not offer that kind of coverage under current rules.
The distinction is not semantic. Public insurance beneficiaries are excluded. Privately insured patients may lose deductible and out-of-pocket maximum credit when they pay cash. California and Massachusetts residents are blocked. The drug list remains limited and still evolving. And the group most directly served — uninsured patients — includes many people for whom even a discounted cash price may be unaffordable.
TrumpRx may produce real savings for a defined patient on a defined listed drug. Its clearest practical use is for an uninsured patient who is not in an excluded state, needs a listed medication, and can still afford the discounted cash price. That is a meaningful use case, but it is much narrower than the public phrase “drug discount program coverage” can make it sound.
References
- FACT SHEET: President Donald J. Trump Launches TrumpRx.gov to Bring Lower Drug Prices to American Patients, The White House, February 2026
- TrumpRx: What's the Value for Customers?, KFF
- TrumpRx: What to know about Trump’s new drug pricing website, STAT, February 5, 2026
- Trump Administration Prescription Drug Initiatives: What Employers Should Know, Aon
- Trump expands TrumpRx prescription drug discount program to 800 medications, Fox News, May 2026
- Delivering Most-Favored-Nation Prescription Drug Pricing to American Patients, The White House, May 2025
- TrumpRx Discounts Only One Drug While 22 Million Americans See Costs Rise, Center for American Progress, April 2026
Comments
Join the discussion with an anonymous comment.