The effects of wildfire smoke on outdoor sports events became hard to treat as a niche sports-medicine problem in mid-July 2026, when Canadian smoke pushed Chicago’s AQI to 597, Milwaukee above 600, and Detroit to 414 — levels classified as “Hazardous.” MLB adjusted games, MLS postponed matches, and NWSL games added mandatory hydration breaks as smoke settled over competition sites rather than drifting past them in the background.[1][2]
That scene is a useful entry point, but it is not the most important part. The clinical question is not whether smoke makes an outdoor event look unpleasant, or whether fans should be warned to stay inside. It is whether an athlete who keeps training or competing in that air is receiving the same exposure as a person walking from a parking lot to a clinic entrance. Physiologically, the answer is no.
Outdoor sport changes the dose. During exercise, minute ventilation can rise 10–20 times above resting levels; mouth-breathing reduces the filtering role of the nose; and higher cardiac output moves inhaled pollutants through the body more rapidly.[3] That is the part that gets lost when a sideline decision is reduced to a single AQI number. The athlete is not just standing in smoke. The athlete is pulling more of it deeper into the respiratory tract, at speed, while the cardiovascular system is already under load.

Why Exercise Makes Smoke Exposure Different
Wildfire smoke is not a generic inconvenience layered on top of sport. Its fine particulate matter, especially PM2.5, can carry a mixture of combustion products and environmental material. Stanford researchers, along with work discussed by Patel and Burke, have described wildfire PM2.5 as potentially about 10 times more toxic per microgram than fossil-fuel PM2.5, with concern tied to polycyclic aromatic hydrocarbons, heavy metals, and biological particles such as pollen and mold.[4] That estimate should not be treated as if it came from one clean head-to-head randomized trial. It is a synthesis-level warning that equal mass does not necessarily mean equal biological effect.
For a resting adult, inhalation still matters. For a runner, rower, soccer player, cyclist, or field-hockey midfielder, the exposure is mechanically amplified. The ventilatory demand of exercise increases the volume of smoky air entering the lungs. As intensity rises, many athletes shift from nasal breathing to mouth-breathing, which bypasses part of the upper airway’s particle-filtering function.[3] The lower airway then sees more particles, delivered faster, with less preconditioning by the nose.
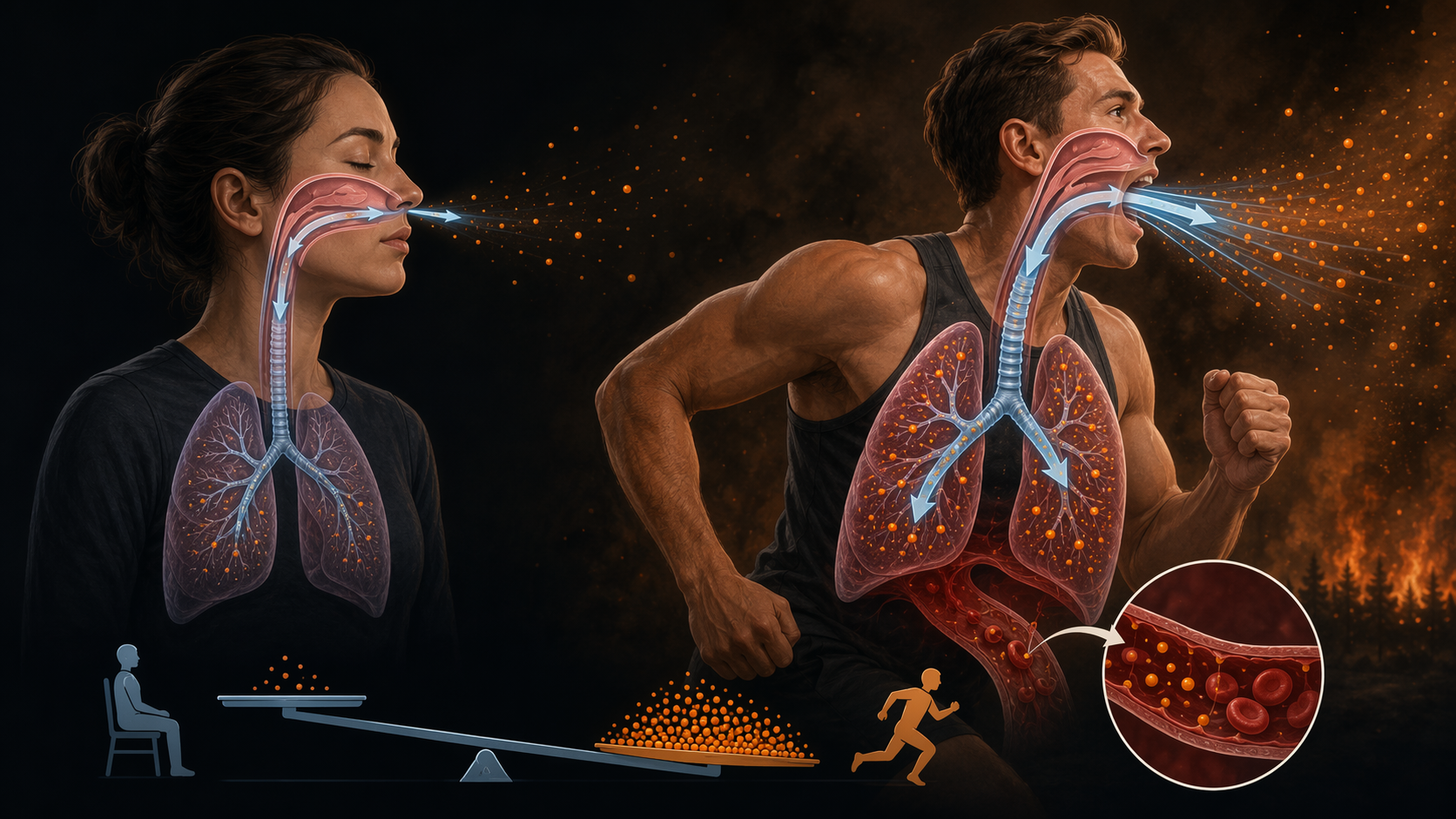
The circulation is not passive in this process. Exercise raises cardiac output to supply working muscle. If inhaled smoke constituents trigger pulmonary inflammation, oxidative stress, endothelial dysfunction, or autonomic imbalance, the system receiving those signals is already operating at high throughput. This is why an endurance session in smoke cannot be judged as a longer version of sitting near smoke. The exposure route, volume, and systemic distribution are altered by the act of exercise itself.
Readers who need a broader primer on PM2.5 and wildfire toxicology can start with What Are the Health Effects of Wildfire Smoke? The sports-specific issue is narrower: during exertion, the same ambient concentration can translate into a different internal dose.
Controlled Exposure Studies Show Acute Physiological Changes
The most relevant evidence comes from controlled human exposure work because it puts exercise and smoke in the same experimental frame. In a 2025 study described by exercise scientist John Quindry and colleagues, 20 healthy participants exercised for two hours in simulated wildfire smoke. The investigators measured immediate declines in vascular endothelial function and autonomic nervous system regulation, with changes detectable within minutes after exposure.[3]
Those endpoints matter because they sit upstream of the clinical events clinicians worry about. Endothelial function reflects how well blood vessels dilate and respond to physiologic demand. Autonomic regulation helps govern heart rate, vascular tone, and the balance between sympathetic and parasympathetic activity. A transient decline after a controlled exposure does not prove that a healthy athlete will develop a cardiac event during a smoky practice. It does show that the cardiovascular system registers the exposure quickly, and in measurable ways, even among healthy participants.
The SToVES study adds another piece of short-term vascular evidence. After wood smoke exposure, participants had elevated pulse wave velocity and central pulse pressure within 24 hours.[3] Pulse wave velocity is commonly used as a marker of arterial stiffness; central pulse pressure reflects pressure load closer to the heart and central arteries. Again, the point is not to overconvert a laboratory endpoint into a sideline rule. The point is that smoke exposure can produce near-term changes in vascular function that are not limited to coughing, eye irritation, or a subjective sense of poor air.
| Evidence source | Exposure setting | Observed change | What it supports |
|---|---|---|---|
| Quindry et al. 2025 | Two hours of exercise in simulated wildfire smoke among 20 healthy participants | Immediate decline in vascular endothelial function and autonomic regulation | Exercise in smoke can produce measurable acute vascular and autonomic effects |
| SToVES | Wood smoke exposure | Elevated pulse wave velocity and central pulse pressure within 24 hours | Smoke exposure can affect near-term vascular stiffness and central pressure |
The strength of these studies is their physiological specificity. They do not rely on a post-event survey asking whether athletes felt irritated. They measure vascular and autonomic responses after defined exposure windows. Their weakness is also clear: the exposure windows are short, the participant groups are small, and the conditions are laboratory approximations rather than full seasons of training, travel, competition, recovery, and repeated smoke events.
The Epidemiology Points in the Same Direction, But It Is Not Athlete-Specific
Population-level cardiovascular data broaden the concern. A 2024 American Heart Association review in Circulation Research reported that cardiovascular morbidity and mortality can surge within three days of wildfire events. The same review described evidence from the 2020 West Coast wildfires in which cardiac arrest and ischemic heart disease emergency department visits increased 42% within 24 hours of dense smoke exposure.[5]
This kind of evidence cannot be laid directly over a roster. General-population emergency department visits include older adults, patients with known cardiovascular disease, people with limited access to filtration, and many others whose baseline risk differs from a trained collegiate or professional athlete. But the timing matters. When cardiovascular morbidity rises within days — and in some analyses within 24 hours — it becomes harder to dismiss the laboratory signals as biologically interesting but clinically irrelevant.
For clinicians, the convergence is more persuasive than any single line of evidence. Controlled exposure studies show acute vascular and autonomic changes under defined conditions. Epidemiological studies show short-lag cardiovascular morbidity during wildfire smoke episodes. Exercise physiology explains why athletes may receive a higher internal dose at the same ambient concentration. Those are three different ways of approaching the same concern, and they point toward acute risk without proving every downstream outcome in every sport.
The general epidemiological literature, including monitoring and prediction approaches, is covered more broadly in Health Risks of Wildfire Smoke and AI Air Quality Monitoring and How Well Does AI Predict Wildfire Smoke Health Effects? For sports medicine, the central unresolved question is not whether smoke is associated with harm in populations; it is how much extra risk is created when high ventilation and repeated exertion are added.
Performance Effects Are Plausible, but Health Endpoints Are the Stronger Evidence
It is tempting to make this a performance story: smoke makes athletes slower, less efficient, or more likely to underperform. That may be true in many real settings, especially when respiratory irritation, perceived exertion, and reduced air quality collide with competition intensity. But the more defensible evidence base in the available literature is cardiovascular and autonomic, not a clean sport-performance dataset with sport-specific outcomes.
That distinction matters in clinical conversations. A coach may ask whether a training session will be useful. An athlete may ask whether symptoms are dangerous. An athletic trainer may have to decide whether a match should continue before symptoms become obvious. The controlled studies do not answer all three questions. They do support a more cautious framing: absence of visible distress during smoky exercise should not be mistaken for absence of physiological effect.
This is especially relevant for endurance and intermittent high-intensity sports, where athletes may cycle repeatedly between heavy exertion and partial recovery. A player who looks functional between shifts, substitutions, or intervals may still be accumulating exposure during each high-ventilation bout. The physiology does not wait for a dramatic collapse to begin changing.
Why the Question Is Becoming Harder to Avoid
The sports disruption in July 2026 was not an isolated scheduling nuisance. Wildfire smoke exposure has become a recurring seasonal problem across wider regions, including places far from the flames. Climate Central reported that at least 164,000 premature deaths in the United States from 2006 through 2020 were attributable to wildfire smoke PM2.5, with climate change contributing about 15,000 of those deaths.[6] Stanford ECHO Lab and Climate Central analyses also reported that per-person exposure during 2020–2024 was four times higher than during 2006–2019.[6]
Those burden estimates are not athlete studies, and they should not be used as if they quantify the risk of one smoky cross-country season or one professional match. Their value here is different. They explain why the sports medicine question keeps returning. More smoke days mean more practices, meets, matches, and races in which clinicians are asked to decide whether outdoor exertion is acceptable under conditions that were once treated as exceptional.
The operational pressure is real. Cancellations carry competitive, financial, travel, and educational consequences. But physiological risk is not erased because postponement is inconvenient. When air quality deteriorates, the decision-maker closest to the athlete has to think in terms of dose, intensity, duration, susceptibility, and recovery — not just the optics of whether the sky looks smoky enough to stop play.
The Evidence Boundary
The current evidence supports a restrained but serious conclusion: outdoor exercise in wildfire smoke is biologically different from passive ambient exposure, and measurable acute cardiovascular and autonomic effects are credible within hours. That is already enough to reject casual reassurance based only on the fact that an athlete is young, fit, or asymptomatic at warmup.
What the evidence does not yet support is a definitive clinical rule for every athlete, sport, exposure pattern, and season. The field lacks athlete-specific longitudinal cohort studies. Current exercise-specific claims rely on short controlled exposures, often around one to two hours, or on extrapolation from general-population epidemiology. Recovery kinetics between repeated seasonal exposures remain unknown. The available controlled-exposure literature also lacks sex-disaggregated analyses, limiting confidence about whether responses differ by sex.
That gap is not academic. A single smoky workout, a week of modified practices, a tournament played under shifting plumes, and several wildfire seasons in a row are different exposure problems. Current studies can show acute vascular and autonomic changes after defined smoke exposure. They cannot yet quantify the cumulative health cost of a season of outdoor training in a region with recurring smoke.
For now, the most defensible clinical posture is to treat smoke during exercise as a dose-amplifying exposure rather than an ordinary environmental backdrop. The athlete’s own physiology — the ventilation, the mouth-breathing, the cardiac output that sport demands — is part of the hazard calculation.
References
- Live updates: Sports schedules altered by wildfire smoke, air quality — USA Today, July 16, 2026.
- Wildfire smoke sports games canceled stay inside — Fortune/AP, July 17, 2026.
- Wildfire smoke can make your outdoor workout hazardous to your health — The Conversation.
- What we know about the health effects of wildfire — Stanford Report, January 2025.
- Impact of Wildfires on Cardiovascular Health — Circulation Research, 2024.
- Climate Change Worsens Wildfire Smoke — Climate Central, 2025.
Comments
Join the discussion with an anonymous comment.