The health case for AI in wildfire risk prediction starts in the lungs, not in the model architecture. Long-term exposure to wildfire smoke PM2.5 was estimated to contribute about 11,415 nonaccidental deaths each year in the contiguous United States, with a 95% confidence interval from 6,754 to 16,075 deaths. That estimate represented about 16.8% of all-source PM2.5-attributable deaths in the study’s analysis, a scale large enough to make smoke forecasting part of health protection rather than a niche environmental service.[1]
That distinction matters because wildfire smoke is not merely another bad-air episode with a different source label. Stanford researchers reported that wildfire smoke was approximately 10 times as toxic as fossil-fuel air pollution per unit mass, a finding that makes the common habit of treating all PM2.5 as interchangeable look clinically too tidy.[2] The exact risk carried by a given plume still depends on exposure, chemistry, dose, duration, and vulnerability. But if the particles are more harmful per unit mass, then a forecast that arrives early enough to reduce exposure may carry more health value than a generic air-quality alert sent after the waiting room is already full.

Where a Forecast Becomes a Health Intervention
A wildfire forecast does not protect anyone by being elegant. It becomes protective only when it changes a decision while there is still time to act: a public health officer issues a smoke advisory before the plume arrives; a school shifts outdoor activity indoors; a dialysis center checks filtration; a hospital reschedules elective cases before operating rooms collide with ventilation constraints; a person with asthma avoids a high-exertion commute.
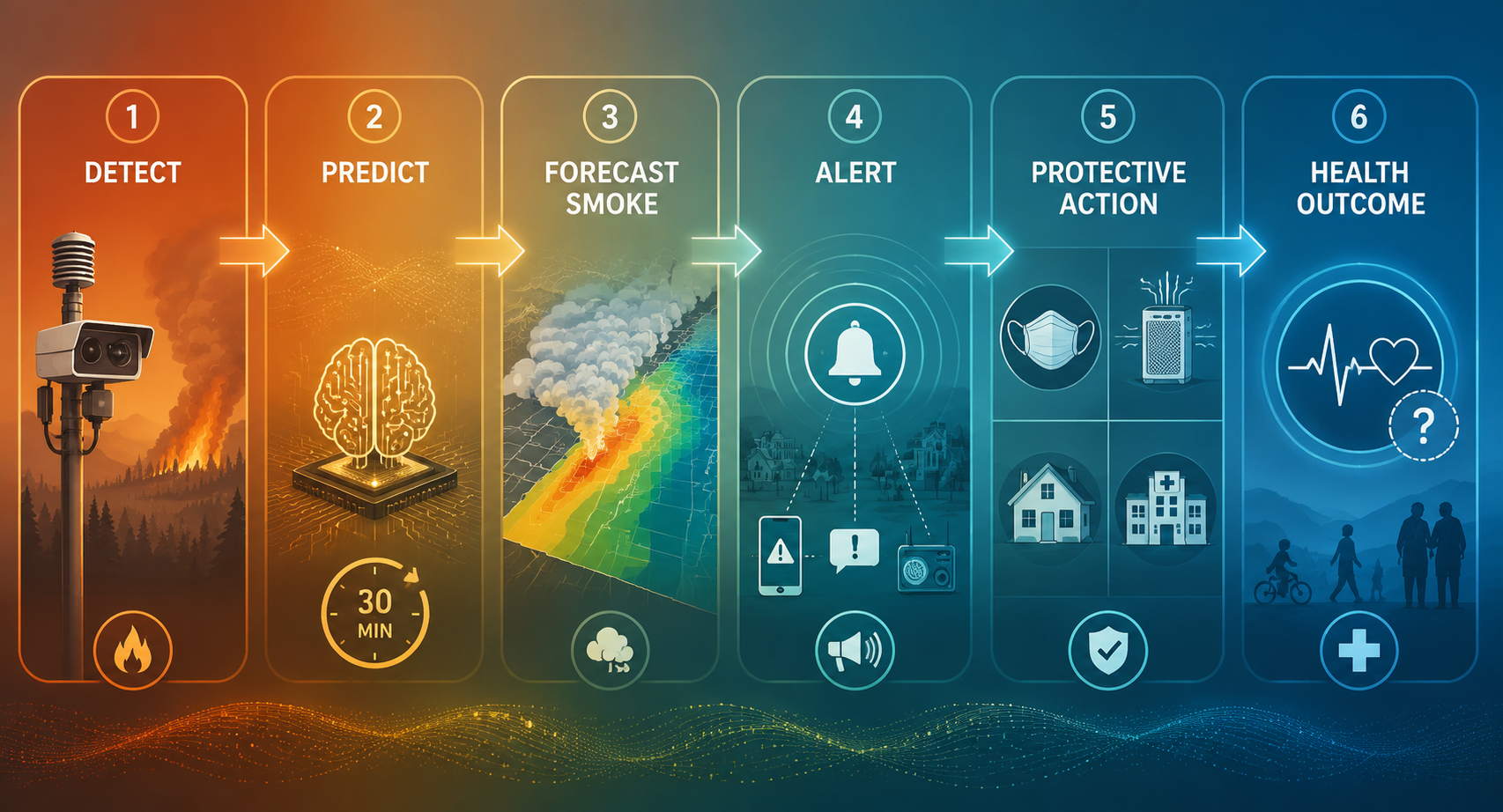
The detection-to-health chain is therefore longer than many technology claims imply. Fire detection, fire spread modeling, smoke dispersion forecasting, exposure estimation, public alerts, institutional decisions, and individual behavior all have to connect. A weak handoff at any point can turn a better forecast into a better-looking dashboard rather than a lower-risk day.
| Link in the chain | What has to happen for health protection |
|---|---|
| Detect | Identify ignition, fire growth, or dangerous conditions early enough to matter. |
| Predict | Update risk estimates as fuels, weather, terrain, and fire behavior change. |
| Forecast smoke | Translate fire behavior into likely PM2.5 movement, timing, and duration. |
| Alert | Deliver information to public health, clinical, and community decision-makers. |
| Act | Change exposure, filtration, masking, evacuation, staffing, scheduling, or outdoor activity. |
| Measure outcome | Assess whether morbidity, mortality, or healthcare disruption actually declined. |
Healthcare operations expose the weak points in that chain quickly. Smoke is not only a population exposure; it is a constraint on care delivery. A hospital may be able to keep its doors open while still facing a narrower margin for elective surgery, respiratory triage, staff commuting, and HVAC-dependent infection-control routines. A concrete example is the use of AI smoke forecasts to prevent emergency surgery cancellations, where the relevant achievement is not that the plume was plotted beautifully, but that teams could move cases before poor outdoor air created a last-minute operating-room problem.
What AI Adds to Wildfire Prediction
The strongest performance claim in the available evidence is not that AI has solved wildfire forecasting. It is narrower and still important: AI-based systems can update wildfire danger every 30 minutes rather than once daily, with reported forecasting performance improvements of 10% to 30% in Australian validation work described by Ardid and colleagues.[3] For health systems, that update frequency is not a technical footnote. A once-daily risk product may miss a fast-changing afternoon wind shift; a 30-minute cycle can give public health and clinical teams a more usable clock.
The caution is geographic and operational. Australian validation does not automatically transfer to North American forests, chaparral, grasslands, peat, urban-wildland interfaces, or mountain meteorology. Fuel type, fire behavior, smoke chemistry, and weather regimes matter. A 10% to 30% improvement in one setting is evidence of real modeling progress, not a guarantee that every health department can plug in the system and expect the same gain.
Still, faster forecasting has a plausible health pathway. If risk updates arrive while roads are open, patients are reachable, and clinics can still change schedules, the forecast can alter exposure. If updates arrive only after smoke has settled into neighborhoods and hospitals have already staffed for an ordinary day, the same information becomes situational awareness rather than prevention.
Detection systems add another layer. NOAA’s Next Generation Fire System combines satellite observations, artificial intelligence, and other science tools to provide fire alerts within one minute of satellite detection, according to the agency’s release.[4] Camera networks and AI-assisted visual detection can also shorten the interval between ignition and response. Those minutes matter most when they are converted into suppression, evacuation, smoke guidance, or healthcare preparation, not when they are counted as an endpoint by themselves.
Smoke Forecasting Is the Health-Relevant Middle
For health readers, the most important word is not only “wildfire.” It is also “health.” A fire-risk model tells officials where burning may occur or intensify. A smoke model tells them who may breathe the consequences, when, and for how long. The health use case depends on that translation from flame behavior into ambient PM2.5 exposure.
This is where AI-supported smoke duration, dispersion, and exposure models become more than technical accessories. They can help estimate whether a community is facing a short smoke pulse, a multi-day episode, or recurring plumes that may strain respiratory services. Readers who need the modeling details can follow the companion review of AI models for predicting wildfire smoke duration and health effects. In practice, the downstream question is usually simpler: does the forecast create enough lead time to reduce dose?
Dose reduction can look mundane. It may mean moving outdoor labor, canceling a youth sports practice, opening a cleaner-air shelter, distributing respirators, switching HVAC settings, placing portable filtration in high-risk areas, or asking patients with cardiopulmonary disease to avoid exertion during a predicted plume. For athletes and exercisers, the exposure problem is especially direct because ventilation rate rises with exertion; the clinical implications are discussed in why exercising in wildfire smoke poses unique health risks and in applied tools for real-time athlete exposure management. Those are downstream examples, but they show why timing changes health relevance.
The Evidence Is Stronger Upstream Than Downstream
The evidence base is not evenly strong across the whole chain. Epidemiology strongly supports wildfire smoke PM2.5 as a serious health burden, with thousands of estimated excess deaths each year in the United States.[1] Toxicity evidence strengthens the concern that wildfire particles may be unusually harmful per unit mass.[2] AI forecasting evidence supports faster and more accurate risk prediction in at least some validated settings.[3] Detection programs show that AI and satellite systems can accelerate identification and alerts.[4]
The thinner evidence begins where many public claims become most confident: the claim that an end-to-end AI wildfire prediction system has already reduced population mortality or morbidity. That conclusion would require more than showing faster detection or better forecast accuracy. It would require evidence that alerts changed behavior or operations, that those changes reduced exposure, and that reduced exposure translated into fewer hospitalizations, exacerbations, deaths, or canceled services compared with a credible counterfactual.
This does not make the systems unimportant. Public health often acts before randomized proof is available, especially when the exposure is widespread, the plausible harm is large, and the protective actions are relatively low risk. But the distinction matters for administrators deciding what to buy, researchers deciding what to measure, and public agencies deciding how to communicate uncertainty. Model performance is an input. Health protection is the outcome.
What Health Systems Should Ask of AI Wildfire Tools
For hospitals and public health departments, the practical evaluation should start with the decision that needs lead time. A respiratory clinic may need a day to adjust staffing. A perioperative service may need enough notice to shift elective cases without causing a separate access problem. A county health officer may need confidence about plume timing before issuing a public advisory. A school district may need morning information, not an afternoon correction.
- What decision will change if this forecast arrives earlier?
- How much lead time does that decision actually require?
- Which population is most vulnerable to a wrong forecast or a missed alert?
- Does the system forecast smoke exposure, or only fire danger and detection?
- Who is responsible for translating the alert into masking, filtration, scheduling, sheltering, evacuation, or clinical triage?
- What outcome will be audited after the event: forecast accuracy, alert timeliness, exposure reduction, healthcare disruption, or health events?
Those questions keep procurement and implementation tied to harm reduction. A tool that improves ignition detection may be valuable for emergency response but insufficient for hospital planning if it does not connect to smoke dispersion. A smoke forecast may be scientifically impressive but operationally weak if it arrives in a format that no clinic, school, or emergency manager is prepared to use. A public alert may be timely but inequitable if high-risk residents lack clean indoor air, transportation, respirators, or the ability to stay home.
The Honest Boundary
AI in wildfire risk prediction and health is best understood as a promising early warning infrastructure, not as a proven population-health intervention in the full causal sense. The case for using it is serious: wildfire smoke PM2.5 is linked to a large mortality burden, wildfire particles may be more toxic than conventional PM2.5 comparisons imply, and AI systems can improve the speed and accuracy of risk updates in ways that plausibly create more time for protective action.[1][2][3]
What has not yet been shown in controlled end-to-end studies is that deploying AI wildfire prediction systems reduces population-level mortality or morbidity. That is the evidence boundary. The next health question is not whether faster forecasts are impressive; it is whether they reliably change exposure, care continuity, and clinical outcomes for the people breathing the smoke.
References
- Long-term exposure to wildland fire smoke PM2.5 and mortality in the contiguous United States, PNAS, 2024.
- Assessing wildfire health risks, Stanford Report, January 2025.
- AI tool predicts wildfire danger faster than current systems, PreventionWeb.
- NOAA unveils powerful convergence of AI and science with revolutionary Next Generation Fire System, NOAA.
Comments
Join the discussion with an anonymous comment.